Annals
of the M.B.C. - vol. 1° - n° 1 - September 1987
ANALYSIS OF 745 HOSPITALIZED BURN PATIENTS
Haberal M., Oner 1, Bayraktar U., Bilgin
N.
Hacettepe University Hospital
Burn Center & Turkish Transplantation & Burn Foundation Hospital, Ankara, Turkey
SUMMARY. From 1 January 1979 to 1 January 1987, 745 burned patients were
hospitalized. Of the patients, 55.84 per cent were under 15 years old (birth to 6 years:
70.20 per cent; j-15 years: 29.80 per cent) and 44.16 per cent were over 15 years. The
causes of burns in the over 15 years gioup were: Flame, Electrical, Scalding, Liquefied
petroleum (LP), Gas explosion and others. The burn causes in the under 15 years group
were: Scalding, Flame, Electrical, Hot meals, and others. After being resuscitated, these
patients were treated with systemic antibiotics, local chemotherapy and
silver-nitrate-incorporated amniotic membrane. Despite all medical efforts, 255 (34.h per
cent) of the hospitalized patients died as a result of various complications.
The burn injury is one of the
nain medical and socio-economical problems for all society but the number of victims may
vary from country to country (1,4).
In our centre, approximately 100 persons are hospitalized as a result of bum injary each
year but fortunately the majority of burns are oiil~ ininor or moderate (2). However the
subject ef buin injury is of world-wide concern for physiciam and licaltli-care personnel
as well as for the victiri from a psychosocial, economic and emotional point ggview.
Therefore, burn treatment should he dea t with by a team, organizing prevention,
rehabilitation and collective education programmes on a national as well as on an
international basis.
Material and Method
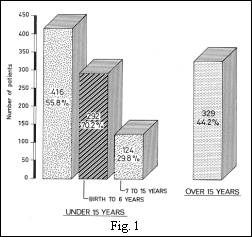
From January 1, 1979 to January 1,
1987, 745 patients were treated in our burn ce-nter as a result of different types of burn
injuries (Fig. 1). Of these, 416 (55.84%) were under 15 years old, 329 (44.16%) over 15
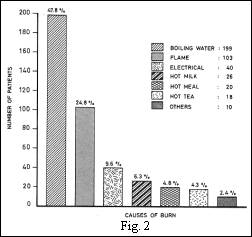
years old. Of 416 patients, 292 ('70.20%) were from birth to 6 and 124 (29.86%) between 7
to 15 years old. The main causes in this group was as follows: Boiling water 199 (47.83%),
Flame 103 (:4.75%), Electrical 40 (9.6%), Hot milk 26 (6.25%), Hot tea 18 (4.32%), Hot
meal 20 (4.8%), others 10 (2.4%): Steam, Lime, Hot Coal, Hot grease, Gun powdcr and one
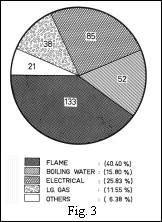
patient was Steven Johnson Sendrourn (Fig. 2). In the 2nd group (over 15 years) the main
causes of burn were as follows: Flame 133 (40.4%), Electrical 85 (25.83%), Boiling water
52 (15.80%), L.P. gas 32 (9.72%) and others 21 (6.38%): Lightning, Hot soil, Chemical, Hot
metal, Steam, Lime, Hot grease (Fig. 3).
All of our patients
were trea,led with Parkland formula, namely, lactated Ringef's solution, given during the
first 24 hr, 2-3 cmł/Kg,/percentage burn. The amount of fluid given should be calculated
from the time of injury and not from the time of admission to hospital. In monitoring,
0.5-1.0 cmł of urine per/kg of body weight/h represents an adequate output, and these
patients should be followed closely for the first 24 hr in case of early complications.
During the second 24 hr period, if the patient cannot be nourished orally, plasma is
administered according to the patient's weight augmented by at least 1 gr of protein per
kg and providing that the patient is responding well to treatment, he or she should be
mobilized as soon as possible.
The three methods that we use in moderate and severe burn wound care are: open method,
dressing and biological dressing methods. Mafenide acetate (Sulfamylon) cream is generally
used for open wound treatment in many centres as well as our own center. When severe
infection is observed, we use silver sulphadiazine and sulfarnylon alternately to decrease
the growth of resistant bacterial colonies, and in infants and the elderly to decrease the
side-effects of sulfamyIon. Silver sulphadiazine is applied 1-2 mm thick under a fine mesh
gauze, along with a bulk dressing.
Since 1978, we have been using 0.5 percent silver-nitrate-incorporated amniotic membrane
(SNIAM) as a biological dressing (3). After the application of SNIAM, the dressing should
be monitored closely for any signs of fluid collections and the presence of pus. If either
one or both are present, the dressing should be changed, otherwise it should be left alone
until healing takes place.
Results
Altogether only 15.4 per cent of the
burn patients were hospitalized and 55.84 per cent of these were under 15 years of age
with the majority also (70.20 per cent) being between birth and 6 years old. In this
group, the main cause of injury was scalding, whereas in the adult group flame and
electrical injury were the leading causes. In comparing times of injury, we found that
there was no seasonal difference in the incidence of burn injury in either the children or
adult groups.
Results of burn wound cultures taken from 745 patients are shown in Table I. The following
bacteria were diagnosed: pseudomonas 40.4%, mixed bacteria 25.6% (pseudomonas, E. coil,
proteus, enterobacter), pseudomonas + E. coil 4.8%, pseudomonas + proteus 3.6%,
pseudomonas + staphylococcus 3.2%, staphylococcus aureus (+) 8.9%, E. coil 5.7%,
staphylococcus aureus (-) 6.4%, staphylococcus aurcus (-) + E. coil 1.4%.
During treatment of the hospitalized burn patients, we encountered the following severe
complications in 267 patients (26.9%): sepsis, acute renal failure, g.i. bleeding,
myocardial infarction, massive necrosis of the small intestine, pulmonary embolus and
adult respiratory distress syndrome (ARDS) (Table II).
| Bacteria |
N° |
% |
Pseudomonas
Mixed bacteria *
Pseudomonas + E. coil
Pseudomonas + proteus
Pseudomonas + staphylococcus
Staphylococcus aureus (+)
E. coil
Staphylococcus aureus (-)
Staphylococcus aureus (-) + E. coil |
301
191
36
27
23
67
43
48
9 |
40.4
25.6
4.8
3.6
3.2
8.9
5.7
6.4
1.4 |
* Pseudomonas, E. coli, proteus,
enterobacter;
+ = Coagulase positive, - = Coagulase negative. |
| Complication |
N° |
% |
Sepsis
Acute renal failure
G.i. bleeding
Sepsis + G.i. bleeding
G.i. bleeding + acute renal failure
Myocardial infiarction
Massive necrosis of small intestine
Pulmonary embolus
Adult respiratory distress syndrome |
184(178)
57(40)
4(2)
8(7)
4(4)
3(3)
1(1)
1(1)
5(5) |
26.9
9.0
0.6
1.1
0.6
0.9 |
Figures in parentheses = patients who
died. |
| Table I - BURN
WOUND CULTURE RESULTS IN 745 PATIENTS |
Table II - ANALYSIS OF SEVERE COMPLICATIONS LEADING TO DEATH IN 241 OF THE 267
HOSPITALIZED PATIENTS |
|
The overall mortality rate in this study was 34.22%
(241 patients) due to different cause;: 66.66% seps is, 14.98% acute renal failure,
2.620/( sepsis and g.i bleeding 1.49%, g.i. bleeding and acate renal failure, 0.74% g.i.
bleeding alone and 3.74% others which include: massive intestinal necrosis (I patient) and
myocardial infaction (I patient) and 5 patients with ARDS.
Discussion
Today, burn trauma is one of the most important problems of our society, but
fortunately most injuries are minor, requiring brief or no hospitalization. We also
observed that most burn patients in the hospitalized groups were children aged from birth
to 6 years old, the major cause of injury being scalding. This could be attributed to lack
of parental supervision and improperly placed heating devices in kitchens and bathrooms
where children roam carefree.
In adults, flame and electricity were the major causes of injury. We believe the injuries
were due to inattentiveness, lack of knowledge in recognizing the danger signs of fire
hazards as well as misusing LP gas and starting fires with flammable fluids improperly.
Besides systemic therapy, for many years we have been using 0.5%
silver-nitrate-incorporated amniotic membrane (SNIAM) as a biologic dressing. Our
experience showed that SNIAM was more effective when used alternately with local
chemotherapy agents such as sulformylon and silvaden.
Pseudomonas were the most important bacteria diagnosed on the burn wound cultures; the
second group was mixed bacteria including pseudomonas, E. coil, proteus and enterobacter.
Sepsis was found to be one of the main complications encountered in hospitalized patients
suffering from flame burns, whereas renal failure and musculoskeletal complications
followed electrical injuries. Unfortunately, burn injuries in Turkey are increasing in
number and claim hundreds of innocent lives every year. In order to prevent this
life-threatening event, measures should be taken by health-care officials and physicians
to educate the public on burn prevention through every available means of communication.
RÉSUMÉ. Du 1 er
janvier 1979 au ler janviç r 1987, 745 patients ont été soignés dans notre centre de
brűlés avec différents types de. lésions par brűlure. De ces brűlés, 416 (55,84%)
avaIents moins de 15 ans et 329 (44,16%) plus de 15 ans. Des 416 jeunes patients, 292
(70,20%) allaient de la naissance ŕ Page de 6 ans, 124 >,86%) de 7 ŕ 15 ans. Les
principales causes des brűlures dans le groupe de moins de 15 ans étaient les suivantes:
eau bouillante 199 (47,83%), flamme 101 (24,27%), courant électrique 42 (10,09%), lait
chaud 26 (6,25%), thé chaud 18 (4,32%), nourriture chaude 20 (4,8%), divers 10 (2,4%),
vapeur d'eau, chaux, charbons ardents, graisse chaude, poudre ŕ fusil, un des patients a
été Steven Johnson Sendroum. Dans le 2' groupe (au-dessus de 15 ans) les causes des
brűlures ont été: le feu 129 (39,20%), le courant électrique 100 (30,39%), eau
bouillante 47 (14,28%), gaz 32 (9,72%) et autres raisons 21 (6,38%) comme la foudre, sol
brűlant, produit chimique, vapeur, métal chaud, chaux, graisse chaude. Aprčs avoir
survécu, ces patients ont été soignés avec des antibiotiques, une chimiothérapie
locale et du nitrate d'argent ircorporé ŕ une membrane amniotique.
Malgré tous les efforts, 255 (34,22%) des 745 patients hospitalisés sont décédés ŕ
la suite de différentes complications.
CONCLUSION: malheureusement,
le problčme des brűlures dans notre pays est en augmentation et il cause des centaines
de victimes chaque année. Pour prévenir ŕ ce type de menace sur la vie, il faudrait que
les autorités s'occupent de la santé publique et les chercheurs prennent des mesures
pour instruire la population ŕ travers tous les moyens de communication sur la
prévention des brűlures.
BIBLIOGRAPHY
- Dobrkovsky M.M.: Bum Survivors
Association in Canada. Dial. Transplant. Burn J. 2, (1) 22, 1984.
- Haberal M., Oner Z., Bayraktar U.,
Bilgin N.: Epidemiology of adults' and children's bums in a Turkish bLm center. Burn J. 13
(2): 136, 1987.
- Haberal M., Oner Z., Bayraktar U.,
Bilgin N.: The use of silver-nitrate-incorporated amniotic membrane as a temporary
dressing. Burn J. 13 (2): 159, 1987.
Me Dougal S. and
Slade W.: Comprehensive Manuals of Surgical Specialities Manual of Burns. Berlin,
Springer-Verlag, p. 3, 1978.
|