Annals
of the M.B.C. - vol. 1° - n° 2 - September 1988
OUR EXPERIENCE IN TREATMENT OF BURNED PATIENTS
Visentini P., Gozzi., Galla A.
Divisione Chirurgia
Plastica, Ospedale di Udine, Italia
SUMMARY.
A rapid account is given of the changing in treatment ofextensively burned patients in the
last twenty years.
A systematic control of blood composition seems of fundamental importance, with particular
regard to protein composition.
Equally important is the appropriate use of antibiotics, an early operation and possibly
remedies which increase immunitary defences. Results obtained with 845 patients are
reported.
During the last
twenty years the treatment of burned patients has been much improved, and owing to this we
have been able to reduce mortality and to better healing quality.
Let us consider this evolution by analysing the modifications of our treatment plan.
Using the older methods we introduced liquids according to some particular formulae (1, 9,
10). The operation was carried out when the burned patient had eliminated eschar and was
covered with granulation tissue (13).
This kind of treatment had the inconvenience of a quite high mortality, a long period of
severe disease and healing with hypertrophic or retracting scars.
The use of lab instruments rapidly making it possible to determine and monitor blood
composition has shown the inadequacy of a therapy based on fixed formulae (1,9,10),
because it was not possible to keep the haernatic composition near normal values.
A factor which, in our opinion, has not been taken into consideration to the right extent
is the proteic composition of the plasma (5, 10, 11). In this relation, one of us (P.
Visentini), when in Padua working on the late Prof. Dogo's team, observed that burned
patients treated exclusively with electrolytes and plasma substitutes frequently showed a
considerable lowering of total proteins (5).
At the beginning we started treating patients in the manner of Batchelor and Birke (2, 3,
10), fundamentally using human plasma for the first two days, and we noticed a
considerable lowering of total mortality (10, 11, 12).
Materials and Methods
We started
regulating the introduction of plasma in the first two days in order to keep haematocrit
and diuresis near normal values. On the following days we introduced the electrolytes, the
albumin and gammaglobulins suggested by the monitor control of different parameters (11).
Using this kind of treatment, the haematic proteins remain near normal values, though
there is a modest lowering in the first two days.
We noted a second advantage when we introduced, from the beginning, antibiotics, which
were changed according to the response of antibiograms on burned tissue and on
haernocultures (8).
In our treatment plan we do not use cannula feeding: all patients eat normally according
to special diets supplying necessary calories. Thus the patients eat what they are used
to.
Normally the patients, even when extensively burned, remained in good general conditions,
and we have introduced, as suggested by Prof. Janzekovic and the Ljubljana and Turin
schools, early intervention (4, 6, 7, 9, 14). We have not found any increase in mortality
but on the contrary perhaps a slight decrease with the advantage of reducing the period of
serious disease and achieving a better healing quality.
More or less a year ago we started changing the ways of operating, applying skin grafts
either treated with mesh-graft or not, by using fibrin glue (Tissucol), without applying
sutures as was used once.
This has allowed us to reduce time of operation and to obtain faster healing.
Results and Conclusions
Re-examining
all the patients treated at the Division of Plastic Surgery at Udine Hospital, we noted a
mortality of 5.3% (Tab. 1), which could partly be ascribed to diseases the patients
suffered from before the burn lesion, but fundamentally because of infections, especially
aflecting old people (Tab. 2).
% Burned body
Surface |
Number of
burned
patients |
Number of
deaths
observed |
| 0 - 9 |
421 |
1 |
| 10 - 19 |
226 |
4 |
| 20 - 29 |
93 |
10 |
| 30 - 39 |
36 |
6 |
| 40 - 49 |
30 |
4 |
| 50 - 59 |
21 |
6 |
| 60 - 69 |
10 |
2 |
| 70 - 79 |
5 |
2 |
| 0 - 89 |
2 |
2 |
| 90 - 100 |
11 |
8 |
| |
845 |
45 (5.3%) |
Tab. 1 - Total number of burned patients admitted to
Udine Hospital from 1973 to 1986, divided according to the extent of 2nd and 3rd degree
burning (Col. 1); total mortality was 5.37%. |
| Age (years) |
% burned
body
surface |
Death/burned |
| 0 - 8 |
15 - 30 |
0 / 52 |
| 31 - 50 |
0 / 5 |
| 51 - 70 |
0 / 2 |
| 71 - 100 |
- |
| 9 - 50 |
15 - 30 |
2 / 97 |
| 31 - 50 |
0 / 35 |
| 51 - 70 |
2 / 16 |
| 71 - 100 |
5 / 19 |
| 51 - 100 |
15 - 30 |
11 / 53 |
| 31 - 50 |
11 / 22 |
| 51 - 70 |
7 / 9 |
| 71 - 100 |
5 / 5 |
Total |
|
43 / 305 |
Tab. 2 - Patients with burns superior to 14% were
divided according to age and extent. It can be seen that mortality is higher in
extensively burned and in old patients. |
|
In trying to
achieve a further reduction of mortality and to better the general conditions of patients,
for some months we have systematically administered a remedy that increases immunitary
defences: the TPI, with results that till now seem satisfactory, though not yet
statistically significant.
In other words, we have tried to change burning from a long disease, with quite high
mortality, to a shorter disease, with the purpose of keeping patients in better general
conditions, so as to be able to operate earlier.
Results are to be assessed not only on the basis of survival, which we hope to improve,
but on the quality of healing, and in this relation we show some cases.
| Fig. 1 |
D.L. aged 2, 2nd and
3rd degree burns on 50% of body surface |
| Fig. 2 |
L. aged 2, same
patient just after healing |
| Fig. 3 |
T.M. aged 18, 2nd
and 3rd degree burns on 50% of body surface |
| Fig. 4 |
T.M. aged 18,
clinically healed |
| Fig. 5 |
C.M. aged 28, 2nd
and 3rd degree burns on 72% of body surface |
| Fig. 6 |
C.M. aged 28, the
patient clinically healed |
| Fig. 7 |
B.A. aged 61, 2nd
and 3rd degree burns on 25% of body surface. Patient's neck is deeply burned |
| Fig. 8 |
B. A. aged 6 1. Neck
treated with skin graft 3 A thickness |
| Fig. 9 |
D.M. aged 5, 2nd and
3rd degree burns on 25% of body surface, particularly on face |
| Fig. 10 |
D.M. aged 5; the
healed child before applying compression garment |
| Fig. 11 |
M.V. aged 28, 3rd
degree burns on 15 % of body surface, particularly on hands and face |
| Fig. 12 |
M.V. aged 28; the
patient's face 2 years after healing |
| Fig. 13 |
M.V. aged 28; a hand
treated with a net skin graft |
| Fig. 14 |
M.V. aged 28; the
hands some years after healing |
| Fig. 15 |
M.V. aged 28; the
hands can move without contracting scars |
| Fig. 16 |
M.V. aged 28; the
hand can easily be closed |
To
obtain these results, collaboration between doctors of the Division and other specialists,
particularly anaesthetists, is necessary; of considerable importance is the work of
nursing personnel and operating theatre staff.
In fact we feel we have to be thankful to these people.
 Fig. 1 |
 Fig. 2 |
 Fig. 3 |
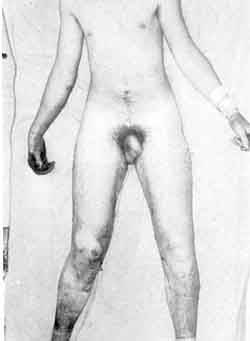 Fig. 4 |
 Fig. 5 |
 Fig. 6 |
 Fig. 7 |
 Fig. 8 |
 Fig. 9 |
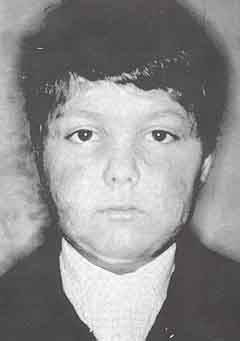 Fig. 10 |
 Fig. 11 |
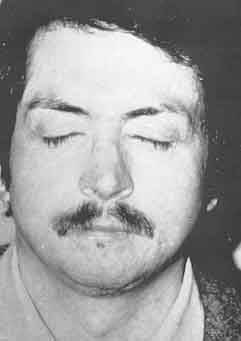 Fig. 12 |
 Fig. 13 |
 Fig. 14 |
 Fig. 15 |
 Fig. 16 |
|
RÉSUMÉ.
Les auteurs considčrent rapidement le changement dans le traitement des brűlés
gravement atteints au cours des vingt derničres années.
Un contrôle systématique de la composition du sang semble d'importance fondamentale, en
tenant compte surtout de la composition protéique.
D'égale importance est l'emploi approprié des antibiotiques, une rapide opération et
peut-ętre des remčdes pour accroître les défenses immunitaires.
Les auteurs font état des résultats obtenus sur 845 patients.
BIBLIOGRAPHY
- Barisoni D.: Le ustioni ed il loro trattamento. Picein,
1984.
- Batchelor A.D.R., Kirk J., Sutherland A.B.: Treatment of
shock in the burned child. - Lancet 1, 123, 1961.
- Birke G., Li1jedalil S.O., Backdahl M., Nylen B.: Studies
on bums - Acta chir. Scand., Suppl. 337, 1, 1964.
- Boswick I.A. Jr.: Chirurgia delle ustioni: La clinica
chirurgica del Nord America, Piecin, 3, 6, 1971.
- Dogo G., Visentini P.: Plasma in anti-shock therapy of
burned patients: clinical findings and considerations. Pharmacological treatment in burns,
Excerpta Medica, 59, 1968.
- Feller I., Grabb WC: Reconstruction and Rehabilitation of
the Burned Patient. National Institute for Burn Medicine, 1979.
- Janzelcovic Z.: The treatment of burns. Burns, 61, 4, 1977.
- Gasparotto A., Visentini R: 11 Cloramfenicolo nel
trattamento locale delle ustioni e delle decorticazioni. Gazzetta Sanitaria 4 10,
- Teich Alasia S., Magliacani G.: 11 trattamento dell'ustione
e dei suoi esiti. Atti dell'incontro intemazionale sulle ustioni, Turin 18-19 June 1982.
- Visentini P.: Considerazioni sulla malattia ustione.
Rivista Italiana di Chirurgia Plastica, 121, 2, 1970.
- Visentini P., Gozzi C, Linda G., Longato F., Paladini E.:
La monitorizzazione della proteinemia nell'ustionato. Rivista italiana di Chirurgia
Plastica, 221, 12, 1980.
- Visentini P., Losasso G.: Ustione ed epatite virale.
Minerva Chirurgica, 417, 38, 1983.
- Visentini P., Martini Z., Boatto U.: Osservazioni
sperimentali e considerazioni cliniche sull'eliminazione dell'escara da ustione. Rivista
Italiana di Chirurgia Plastica, 31, 1, 1969.
- Yong Chili-Chun, Hsu Wei-Shia, Shih Tsi-Siang: Treatment of
Burns. Shanghai Scientific and Technical Publishers- SpringerVerlag, Berlin Heidelberg New
York, 1982.
|