Annals
of the M.B.C. - vol. 1° - n° 2 - September 1988
PRIORITIES AND PITFALLS IN TREATMENT OF BURNS
Zdravic F.
University Department for Plastic Surgery and Burns, Medical Center Ljubljana,
Yugoslavia
SUMMARY. An
analysis of burn work done in I-jubIjana during the last 30 years showed that the most
important lesson we learned is to plan an individual strategy of treatment for each
severely burned patient. It is an advantage to organize the bum service in the country in
erder to have the severely burned patient sent for treatment without delay. If this is
done, then we do not miss the best time to perform releasing incisions or excisions of the
burn eschar in circumferential bums which compromise the blood circulation causing severe
late invalidity.
The early delayed excision of deep dermal burns is the treatment of choice; however it may
produce very bad results if not performed properly. A series of patients is shown to
illustrate these points.
Introduction
It is very
useful to speak openly about our mistakes in early excision of deep dermal and subdermal
burns. Sharing the knowledge about pitfalls is often more instructive than the technical
details describing how to achieve excellent results.
Burn surgery has made great progress, and the active approach to eliminate the necrotic
layers of skin as soon as possible after trauma followed by immediate grafting has won
worldwide acceptance.
Even among surgeons convinced of the advantages of this procedure there might be some who
are overzealous and do the operation at the wrong time.
Discussion
I would
like to present a number of situations which resulted in unexpected complications because
some of the details in the treatment were not respected. The first point 1 would like to
present is the time factor in excision.
When Dr. Janzekovic was working and studying the details of early delayed excision she
suggested excising the burned layers between the third and the fifth day. There are good
reasons for this. As everybody knows a burn will usually be followed by oedema, and the
alterations in the circulation make it therefore difficult to differentiate properly the
viability of tissue.
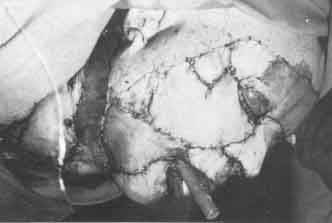
As shown in the slides an overzealous surgeon tries to perform the excision of a deep
dermal burn of the face during the first twenty-four hours. As seen in the first slide
(picture No. 1) there was clearly a great amount of oedema. The excision performed was in
many areas too superficial and had a disastrous result as the grafts which were applied
immediately did not take. Two years of treatment and more than ten operations were
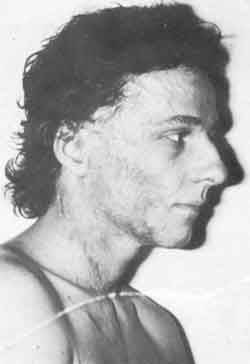
necessary in order to correct the deformity (pictures 2, 3, 4, 5). The conclusion is
clear. Never excise before the oedema has subsided.
 |
Picture No. 2 |
 |
Picture No. 3 |
 |
Picture No. 4 |
 |
Picture No. 5 |
| Unsuccessful
grafting and end result after additional operation |
|
On the other hand in certain cases there are clear indications for
a quick and aggressive surgical approach. If the bum of an extremity is full-thickness and
circular causing constrictions, it is necessary to operate. We would prefer to perform not
incisions but immediate excision in such situations followed by immediate grafting;
provided, of course, that the general condition of the patient permits this procedure,
i.e. that the bum of the extremities is not associated with extensive burns elsewhere. In
such a situation, we should change our strategy of treatment. As regards priorities we are
therefore convinced that immediate excision in constrictive, circular and very deep bums
in extremities followed by immediate grafting is the right choice which will give better
results in a shorter period of time.
A second consideration concerns mesh grafts; their usefulness is generally well-known.
However it is a great mistake to apply mesh grafts to skin defects of the face. The young
boy who was admitted rather late presented granulating infected areas of the face (picture
No. 6) and because of the infection the surgeon was convinced that it would be safer to
cover these areas with mesh grafts and thus obtain a good healing (picture No. 7).
 |
Picture No. 7 |
 |
Picture No. 6 |
 |
Picture No. 8:
End result unsatisfactory |
| Granulating
area of the face - mesh graft applied |
|
This was done, but the
aesthetic appearance was never satisfactory, either immediately after the healing or in
the years that followed. He underwent several abrasions but from the aesthetical point of
view the result, although acceptable, did not completely satisfy the patient (picture No.
8). There is one important observation connected with this case: there seems to be a great
reluctance to excise such areas later and replace them by a skin graft of proper
thickness.
A third consideration concerns early delayed excision of bum of the hand followed by
immediate grafting. In the last twenty years we have performed more than five hundred
cases of early excision of burned hands and it was discovered during that period that
excision under tourniquet required a great deal of experience. It was found that under
inexperienced hands even viable layers of skin were sacrificed unnecessarily. In
performing excision under tourniquet, which we prefer, the surgeon is only guided by the
pearl white appearance of the dermis and by small unobliterated vessels. Therefore it
would be safer for beginners to excise without a tourniquet and be guided by capillary
bleeding as regards the viability of the tissue. However we should not forget that there
is a valid indication for using the tourniquet in all cases where we must save every drop
of blood we can. It is also useful to use magnifying glasses to look at the excised areas
in order to differentiate better the thrombosed and non-thrombosed vessels of the dermis.
Conclusion
These considerations, which all relate to
the technical procedure in treating deep dermal and subdermal burns, demonstrate that it
is not only important to know the method itself, but also all the details and possible
errors in performing these procedures.
RÉSUMÉ. Une
analyse du travail effectué sur les brűlures ŕ Ljubljana au cours de ces 30 derničres
années a montré que la leçon la plus importante ŕ retenir est celle de projeter une
stratégie individuelle pour le traitement de chaque patient brűlé.
C'est un avantage que les patients envoyés soient soignés sans retard. Si cela est fait,
nous ne perdons pas un temps précieux pour pratiquer une incision ou une excision de la
croűte de la brűlure dans le cas de brűlures circonférentielles qui compromettent la
circulation du sang et causent des invalidités graves.
La premičre chose ŕ faire dans le cas de brűlures dermiques profondes est de ne pas
retarder l'excision. Cependant cela pourrait avoir des conséquences pénibles si elle
n'était pas bien faite. Des exemples illustrent ces points.
BIBLIOGRAPHY
- Janzekovic J.: Symposium
on Burns, Maribor, 1968.
|
