Annals
of the M.B.C. - vol. 1° - n° 2 - September 1988
SEVERE ELECTRICAL INJURY AND REHABILITATION
Haberal W Oner 1, Gulay K, Bayraktar U.,
Bilgin N.
Hacettepe University Hospital Burn
Centre & Turkish Transplantation and Burn Foundation Hospital, Ankara - Turkey
SUMMARY. Between
January 1979 and January 1987, 125 patients were treated in our centre as a result of
electrical injuries.
Of these, 85 patients were over 15 years old (89.4% males and 10.6% females) and 40
patients were under 15 years old (92.5% males and 7.5% females).
The occupation of the over 15 years old group was mainly that of electrician, and of
student in the under 15 years old group. Besides systemic and surgical treatment, 5 of our
6 multiple trauma patients were rehabilitated through physical therapy and prothesis and
have returned to their occupation in society.
Human life and
socio-economical activity have changed rapidly since the use of electrical energy has
spread all over the world. In our country, electrical energy is used widely, but
improperly, and because of this the incidence of electrical injury is high, causing .many
severe complications or death (3). This paper will cover our experience with severe
electrical injury.
Materials
and methods
From 1 January 1980 until 1 January 1987, 745 patients were admitted to our Burn
Centre. Of these, 125 (16.77%) had electrical bums (Fig. 1), not including 7 flash bums,
two lightning, and one bum injury from an electrical stove. 85 (68%) of the 125 patients
were more than 15 years of age, the mean age being 29.04 years. 76 (89.40%) of these
patients were males and 9 (10.60%) females. For patients 15 years old or younger the mean
age was 10.54 years. 37 (92.25%) of these patients were males and 3 (7.75%) females with
the majority 11 to 15 years of age (Fig. 2).
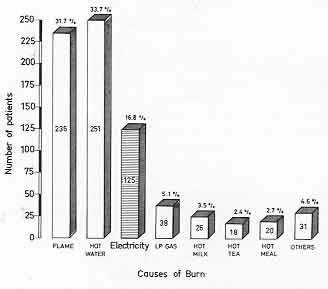 |
Fig.
1 |
 |
Fig. 2 |
|
Fifty-two (44%)
of the patients were injured with domestic electric current (220-400 volts) and 62
(44.68%) were injured with high-tension (1,000-38,000 volts).
The occupations of patients over 15 years were as follows: 36 (42.35%) electricians, 20
(23.5%) bluecollar workers, 9 (10.58%) farmers, 7 (8.23%) housewives, 6 (7%) teachers, and
7 (8.23%) others, including 2 students, 2 chauffeurs, 1 pharmacist, 1 retired person and 1
shoemaker (Fig. 3).
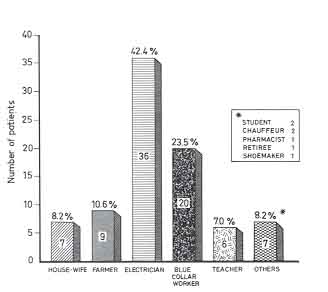 |
Fig. 3 |
|
Five multiple trauma
patients:
A.Y., 26 years old male (farmer):
electrical accident with high voltage 3 extremities 26% 2nd-3rd T.B.S.A.
D.D., 32 years old male (teacher): accident With high voltage 3 extremities 18% 2nd-3rd
T.B.S.A.
S.B., 18 years old female (secretary): accident high voltage 3 extremities 10% 2nd-3rd
T.B.S.A.
G.S., 26 years old female (teacher): accident high voltage 3 extremities 9.5% 2nd-3rd
T.B.S.A.
M.S., 23 years old male (blue-collar worker): accident high voltage 4 extremities 33% 3rd
T.B.S.A.
All of our
patients came to our centre from throughout Turkey, with no seasonal statistical
difference in incidence of injury.
The treatment of all patients began at the time of hospitalization. Following a routine
examination, IV fluid (Saline or Saline with dextrose) was administered, and following the
results of the electrolyte meaArements, provided potassium levels were normal, the
solution was changed to Ringer's lactate. The rate of administration was adjusted
according to urine output of at least 50 nil per hour. If the patient was oliguric and
acidotic, sodium bicarbonate, 20-40 gm of mannitol, and 40-100 mg furosemide were given.
If the patient still remained oliguric, and potassium, BUN and creatinine levels were
rising, peritoneal or haemodialysis using a double lumen subclavian catheter (Gambo
SCK-102 20 cm, Lund, Sweden) was resorted to. We found that this system was very easy to
use for both haemodialysis and parenteral alimentation. A urinary catheter and a central
venous pressure catheter were used only in severe cases or if clinical evaluation so
indicated.
Following initial stabilization, the patients were taken to the dressing room for
re-evaluation and if necessary, debridement, escharatomy, and fasciotomy, and wounds were
cleansed and closed using one of the local chemotherapeutic agents, such as silver
sulphadiazine, mafenide acetate, or silver incorporated amniotic membrane. This procedure
was repeated until all nonviable tissue was removed in cases where amputation was
required. Wounds were then closed whit a skin graft or a flap.
Besides systemic and surgical treatment, 5 of our 6 multiple severe trauma patients were
rehabilitated through physical therapy and prothesis.
Results
These
five patients required a total of 15 surgical procedures (each patient at least two
procedures) which included 6 major upper and 4 major lower extremity amputations. The rest
were minor, such as debridements and grafts.
After completely recovering from acute bum treatment all five patients had a different
number of protheses: one patient required all 4 extremities protheses (blue collar
worker); one right forearm (secretary); one left forearm (teacher); one left below knee
and right above knee (farmer); and one bilateral total upper extremities prothesis
(designer).
At present, all of our five patients are doing very well with their occupations and living
without creating any problem with minimal help in society.
Discussion
Electrical
bum injury is one of the severest problems in our population. The main causes of injury in
the over 15 years old group was misuse, inattentiveness, and lack of knowledge, also the
fact that utility poles and wiring are constructed low and extremely close to buildings,
where even putting up a TV antenna can be life threatening. In the under 15 years old
group, the injuries were mainly a result of mischievous activity that involved climbing,
and lack of parental supervision. Another contributing factor is the lack of control of
the systems by the electric companies.
One of the major complications was musculosketetal, which resulted in most of the major
amputations.
We found that one of the reasons for the high number of amputations could be that early
surgical decompression with fasciotomy and sequential wound debridement (1, 2, 4, 5) was
in many cases not accomplished as early as possible because the patients were transported
to our centre from nonspecialized facilities. Following electrical and other types of bum
injuries physical and occupational therapy must be applied as early as possible to prevent
complications during or after treatment. In our Bum Centre, these methods have been
applied for many years as a daily routine, including severely burn patients also. After
complete recovery the prothesis is adjusted if necessary. While the prothesis is being
prepared, patients have to adapt very well and try to turn back to their near normal or
normal life.
Our experience with five patients showed that the patient with severely electrical injury
and multiple amputation could tolerate this kind of life very well. Therefore, physical
and occupational therapy must be applied as early as possible after electrical injury to
return the patient to his normal life in society.
RÉSUMÉ.
De janvier 1979 ŕ janvier 1987, 125 patients ont été traités dans notre centre ŕ la
suite de blessures dues au courant électrique. De ces 125 malades, 85 avaient plus de 15
ans (89,4% hommes et 10,6% femmes) et 40 avaient moins de 15 ans (92,5% hommes et 7,5%
femmes). Les individus de plus de 15 ans étaient principalement des électriciens tandis
que dans le groupe de ceux de moins de 15 ans il y avaient surtout des étudiants.
En plus du traitement systémique et chirurgical, 5 de nos 6 patients ayant subi de
multiples traumatismes ont recouvré leurs fonctions grâce ŕ une thérapie physique et
des prothčses et ont pu reprendre leur place dans la société.
BIBLIOGRAPHY
- Artz C.P., Moncrief J.A.:
Treatment of Burns. Saunders, Philadelphia, London/Toronto, 1969.
- Burke J.F., Quinby W.C., Bondoc C.
et al.: Patterns of high tension electrical injury in children and adolescents and their
management.
Am. J. Surg., 133:492, 1977.
- Haberal M.: Electrical Bums: A
five year experience - 1985 Evans Lecture. The Journal of Trauma. 26 (2):103, 1986.
- Holiman C.J., Saffle J.R., Kravitz
M. et al.: Early surgical decompression in the management of electrical. injuries. Am. J.
Surg., 144:733, 1982.
Wang Xue-Wei et
al.: Early vascular grafting to prevent upper extremity necrosis after electrical bums:
11. Experience with wound infection management. Bums, 10:179, 1984.
|