| Annals of Burns and Fire Disasters - vol. X - n. 1 - March 1997
CHEMICAL
BURNS - EPIDEMIOLOGY
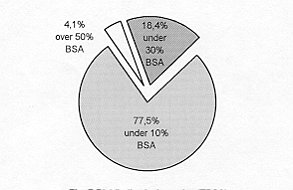
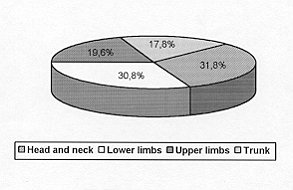
Vaglenova E. Burn and Plastic Surgery Centre, Pirogov Emergency Medical Institute, Sofia, Bulgaria SUMMARY. This survey considers the 5-year period 1991-1995, during which the total number of burn patients admitted to our clinic was 1548. Forty-nine (3.2%) presented chemical burns (38 male/11 female; mean age, 41.4 yr; age range, 14 to 80 yr). The commonest cause of chemical burns was some form of acid. The home was the most frequent site of chemical burn incidents (73.5% of all such cases), the main reasons being criminal acts or negligence. Burn extent ranged from I to 95% TBSA, with a predominance of injuries in less than 10% TBSA. Thirty-six patients (73.5%) presented deep partial-thickness and full-thickness skin loss. The head, face, and neck were affected in 31.8% of the patients, the lower limbs in 30.8%, the upper limbs in 19.6%, and the trunk in 17.8%. Patient mortality in this series was 4. 1 %. Introduction Considering Bulgaria's limited surface
area, chemical industries are well represented. However, our research indicates that
chemical burns are quite rare, constituting only 3.2% of all burns treated in our centre
in the 5-year period 1991-1995. Material Between 1991 and 1995, 1548 adult burn patients were treated in our clinic, of whom 49 (3.2%) presented burns due to chemical agents (Fig. 1).
The annual percentage varied between 1.6 and 5.2% (Table 1).
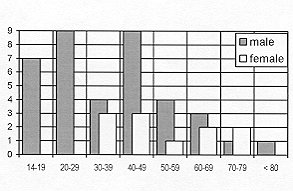
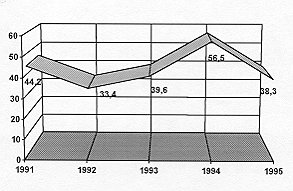
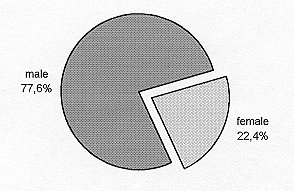
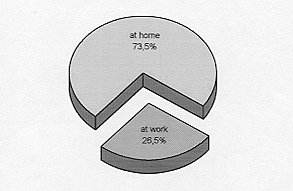
Epidemiological analysis The age of the patients ranged between 14 and 80 yr (Fig. 2). The accidents occurred most frequently to patients of active working age (20-60 yr). The mean age was 41.4 years, varying during the 5-year period from a minimum of 33.4 yr in 1992 to a maximum of 56.5 yr in 1994 (Fig. 3) The male to female ratio was 38:11 (77.6%:22.4%) (Fig. 4). In 36 cases (73.5%) the burns were suffered at home as a result of carelessness or criminal action (Fig. 5). Accidents at work constituted 13 cases (26.5%).
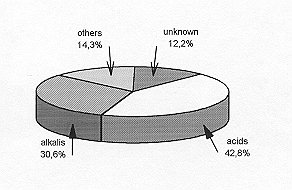
With regard to the cause of the burns,
acids played a primary role (42.8% of cases). Sulphuric and nitric acids were most
frequently involved. Burns caused by bases represent 30.6% of the cases, most frequently
caustic soda (sodium hydroxide). The agent was not definitely established in 12.2% of the
patients (Fig. 6).
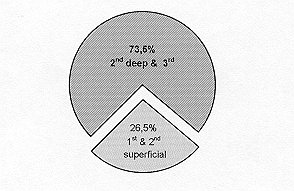
Thirty-six patients (73.5%) presented deep
partial-thickness and full-thickness skin loss, treated by surgery. The remaining thirteen
patients (26.5%) had superficial burns, and epithelialization occurred spontaneously (Fig.
8).
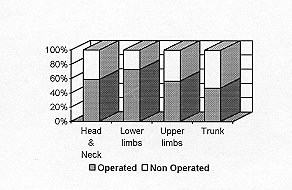
If we consider the localization of the burns and the surgical operations performed on the sites (Fig. 10) it can be seen that the highest percentage of operations was for burns in the lower limbs (72.7%), followed by the head and neck (58.8%) and the upper limbs (57. 1 %).
The mean hospital stay was 27.1 days. Only eight patients (16.3%) were admitted to the centre in the immediate post-trauma phase. The mortality rate in the series was 4. 1 %. Discussion Chemical burn patients treated in our
centre in the 5year period 1991-95 constituted 3.2% of all patients admitted (the
corresponding figure in 1968 was 10.0%). Other authors` give higher percentages for
chemical burns (4.P 13.3%), although we are aware that the data are not absolutely
comparable.
RESUME. Cette étude considère une période de cinq ans (1991-1995) pendant laquelle 1548 patients brûlés ont été hospitalisés dans notre clinique, dont 49 (3,2%) atteints de brûlures chimiques (38 mâles/Il femelles; âge moyen, 41,4 ans; limites d'âge minimum et maximum, 14 et 80 ans). La cause la plus commune des brûlures chimiques était l'acide. La plupart des brûlures dues aux agents chimiques se sont produites à la maison (73,5% des cas), causées principalement par des actions criminelles ou la négligence. L'extension moyenne des brûlures variait entre 1 et 95%, avec une prévalence de lésions en moins de 10% de la surface corporelle. Trente-six patients (73,5%) présentaient une perte cutanée d'épaisseur variable ou totale. Les parties du corps les plus intéressées étaient la tête, le visage, et le cou (31,8% des patients), les membres inférieurs (19,6%), et le tronc (17,8%). Le taux de mortalité de cette série de patients atteints de brûlures chimiques était 4, 1 %. BIBLIOGRAPHY
|