| Annals of Burns and Fire Disasters - vol. X - n. 1 - March 1997
THE ROLE OF
AZTREONAM IN THE CONTROL OF GRAM. NEGATIVE BURN WOUND INFECTION
Kamel A.H.(1), El Megeed E.A.(2)
(1) Plastic and Reconstructive Surgery Unit,
Assiut University Hospital, Assiut, Egypt Microbiology
(2) Department, Assiut University, Assiut
SUMMARY. This
study was conducted on 68 patients with mixed second- and third-degree burns and/or raw
areas admitted to the Burn Unit of Assiut University Hospital and the Assiut Burn Centre
(Egypt). The purpose was to study the effect of topically applied Aztreonarn alone and in
conjunction with its systemic administration in the control of gram-negative burn wound
infection. The results were compared with those of a control group of 57 patients with
gram-negative infection who received a classic method of dressing. Assessment was
performed on clinical and bacteriological bases. It is concluded that the use of
Aztreonam, as a topical dressing is very helpful in the control of gram-negative mixed
second- and third-degree degree burn wound infection, particularly if due to Pseudomonas,
and that in the presence of high fever over 38.5 'C it is advisable to administer
Aztreonarn also systemically.
Introduction
Gram-negative bacteria have assumed a
primary lethal role among the causes of burn wound infection and septicaemia in burn
patients.' They represent 47-65% of the micro-organisms that cause burn wound invasion. A
review of the literature shows that the bacteria isolated from invaded burn wounds were Staphylococcus
aureus (17-30% of cases),Pseudomonas pyocyanea (20-28%), Pseudomonas
aeruginosa (5-28%), Proteus (9-15%), Escherichia coli (4-15%), Streptococcusfaecalis
(2-8%), and Staphylococcus albus (1 -2%)." The presence of mixed wound
infection by more than one micro-organism is a common finding.
The pathophysiology of burn wound infection
In mixed second- and third-degree
burns, early colonization occurs within the lumen of hair follicles and glands.
Colonizations with bacterial growth of less than 101 bacteria per g of tissue are
compatible with survival and healing. When the bacterial counts exceeds 101 the bacteria
spread from the follicles and colonization occurs along the dermal- subcutaneous
junction.' Perivascular colonization is accompanied by thrombosis, vascular occlusion, and
necrosis of any viable tissue.` Partial-thickness burns then convert to full-thickness
lesions as a result of ischaemia and bacterial autolysis. Bacterial growth beyond 10
constitutes burn wound sepsis, and 10 to 10 Pseudomonas organisms per g of tissue
are found in lethal injuries.
Topical therapy in burns
Clearly, early permanent wound closure
should eliminate the hazards of infection.` In patients whose wounds remain open for
several weeks or more, the protracted use of antimicrobial agents is necessary and
represents the single most important means of preventing septic morbidity and death. It is
evident that delivery of systemically administered antimicrobial agents to the deepest and
most severely ischaernic areas of the wound cannot be relied upon, and that the topical
application of antimicrobial agents will best ensure their presence in adequate
concentration, at least on the wound surface where the risk of bacterial contamination is
greatest. Although colonization of the wound can occur by haematogenous spreading from
distant foci, this appears to be the exception rather than the rule.
Deitchet al.11 observed that effective
topical agents possess the following qualities:
they have a broad in vitro spectrum
of activity and are effective against the most commonly isolated organisms
they penetrate the eschar yet are not
appreciably absorbed systemically
they do not possess any significant
local histotoxicity
they have a known absorption rate
they delay colonization for a variable
period measurable in days not weeks
they maintain the wound bacterial count
at a lower level than can otherwise be achieved
Yurt et al.11 emphasized that routinely
used topical agents associated with a high incidence of emergence of resistant organisms
pose a notable problem, particularly in a setting where patient numbers are high and
isolation facilities inadequate.
There are two objections against the use of true antibiotics for topical use: firstly,
that most of them act by inhibiting a specific metabolic pathway rather than at multiple
sites (as most antiseptics do); secondly, that serious systemic toxicity, including renal
and pulmonary failure and toxicity (ototoxicity), has resulted from the topical
application on burns of antibiotics such as neomycin, polymyxin, gentamicin, and
sulphonamide mafenide, owing to their absorption from even relatively small wounds.
What is Aztreonam?
Aztreonain is a monobactam, a new
family of beta lactain antibiotics.` It is selectively active against gram-negalive
micro-organisms and inactive against gram-positives and anacrobes.11 The minimal
inhibitory concentration (MIC) for gram-negative micro-organisms ranges from 0.1 to 50 p
g/ml, and MIC90 ranges from 0.1 to 25 p g/ml."," It is monocyclic and is
therefore easily excreted by the kidney. It has no dangerous effects on renal or hepatic
function.` It has little or no effect on immunity and on phagocytic cell
function."-" Aztreonam can be used safely in doses of up to 8 g per day and for
up to 31 days. It can be given to infants from the age of one week.`
Patients and methods
This study was conducted on 68
patients from the burn unit of Assiut University Hospital and Assiut Burn Centre who were
subjected to dressing with Aztreonarn solution. The patients were selected when the
bacterial culture showed gram-negative infection and the micro-organism showed sensitivity
to Aztreonam. All had mixed second- and thirddegree burns and/or raw areas. The results
from this group were compared with those of the control group, i.e. 57 patients with
gram-negative infection who received a classic method of dressing with antimicrobial
ointments available in Egypt (Betadine, microfurazone, silver sulphadiazine). The data
relative to the two groups are presented in Table L
| |
Aztreonam
group |
Control
group |
T-test |
Number |
68 |
57 |
Mean age (yr) |
19.5 ± 5.0 |
20.1 ± 3.0 |
p>0.05 insignificant |
Sex |
32 m / 36 f |
27 m / 30 f |
p>0.05 insignificant |
TBSA (%) |
16.5 ± 5.0 |
15.2 ± 4.0 |
p>0.05 insignificant |
|
Table I -
Patients' collective data |
|
The study group of 68
patients was divided into two subgroups. The first subgroup (40 patients) received
Aztreonam topically and systemically in their therapeutic dose. These patients were
selected to take Aztreonam by both routes because they had high fever (over 39.5 'C). The
second group (28 patients) received Aztreonam only topically. The data relative to the two
subgroups are presented in Table II.
| |
Topical
and
systemic |
Topical
only |
T-test |
Number |
40 |
28 |
Mean age (yr) |
18.5 ± 5.0 |
20.7 ± 7.0 |
p>0.05 insignificant |
Sex |
20 m / 20 f |
12 m / 16 f |
p>0.05 insignificant |
TBSA(%) |
16.0 6.0 |
18.07.0 |
p>0.05 insignificant |
|
Table II
- Data of patients receiving topical and systemic Aztreonam and only topical Aztreonam |
|
Aztreonam dressing
In the study group we prepared the
Aztreonani solution by diluting a I g vial in 250 ml saline in completely aseptic
conditions (this dilution exceeds the MIC for all gram-negative micro-organisms). After
washing of the wound with saline, or hydrotherapy, we covered the wound with sterile gauze
impregnated in Aztreonarn solution. The second layer consisted of sterile vaseline gauze
to prevent absorption of the Azactam solution by the overlying dressing. The third layer
consisted of sterile cotton. Dressings were performed daily.
Classic dressing
The control group received a classic
dressing. The wound was washed with saline, covered with an antimicrobial ointment
(Betadine, nitrofurazone, or silver sulphadiazinc), and covered with sterile gauze and
cotton. Dressings were performed daily.
The effect of topically used Aztreonarn was monitored clinically and bacteriologically.
Clinically, we recorded local manifestations of infection and the degree of improvement as
well as systemic manifestations of infection (mainly body temperature). The
bacteriological study regarded the cultures and sensitivity before the dressing, and
subsequently every other day in order to determine the type of micro-organism, if present
(i.e. superinfection), and sensitivity to antibiotics. This continued until complete
closure of the wound, usually within 21 days. Bacterial counts were performed before
initiation of Aztreonarn dressing, on days 3, 4 and 5; and immediately before grafting, if
indicated. Two methods of bacterial count were used .29,30
Results
Sixty-eight patients received Aztreonarn
either only topically or together with systemic administration. The effect of topically
applied Aztreonam in the control of grain-negative burn wound infection was studied and
compared with results in the control group (57 patients).
Statistical analysis showed that the study and control groups were similar as regards mean
age, sex ratio, and percentage of burn surface
When Aztreonam was administered only topically, control of local manifestations of
infection was established after 3.8 ± 1.0 days, control of fever to less than 38.5 'C was
established after 4.0 ± 1.0 days, and the bacterial count dropped to less than 10' per gm
of granulation tissue after 4.0 ± 0.4 days. These figures were found to be significantly
reduced compared with those of the control group, in which patients received a classic
method of dressing (Table III).
| |
Aztreonarn
group |
Control
group |
T-test |
Control of local
manifestation (days) |
3.8 ± 1.0 |
10.0 ± 3.0 |
p<0.01 significant |
Control of systemic
manifestation (days) |
4.0 ± 1.0 |
7.0 ± 2.0 |
p<0.05 significant |
Control of bacterial
count(days) |
4.0 ± 0.4 |
9.0 ± 1.5 |
p<0.05 significant |
|
Table III -
Comparison between the effects of Aztreonam dressing and of classic dressing |
|
As already said, the study
group was divided into two subgroups of respectively 40 patients, who received Aztreonarn
topically and systemically, and 28 patients, who received it only topically. There was no
statistical difference between the two subgroups as regards mean age, sex ratio, or mean
burn surface area. Statistical analysis showed that there was a non-significant difference
in the time periods necessary for the control of local manifestations of infection and for
the reduction of bacterial count to less than 101 per gm of tissue whether Aztreonarn was
used topically and systemically or only topically.Systemic manifestations of infection
were significantly controlled earlier in patients who received Aztreonarn topically and
systemically, although this group originally presented high fever.
The bacterial count in this study was performed using two methods, the ordinary and the
rapid. The two subgroups presented identical results (i.e. the bacterial count was found
to be more than 101 per g of granulation tissue by the ordinary method when more than one
micro-organism per field was detected by the rapid method).
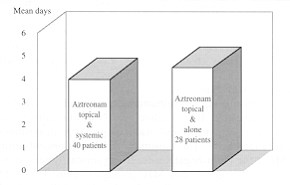 |
Fig. 1 - Control of bacterial
count. T-test p>0.05. |
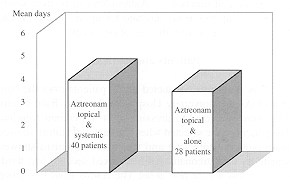 |
Fig. 2 - Control of local
manifestations. T-test p>0.05. |
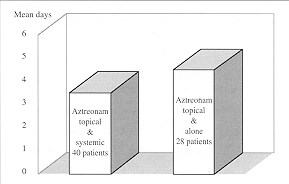 |
Fig. 3 - Control of temperature to
less than 38.5 °C. T-test p>0.05. |
|
Discussion
Success in the topical use of the
antibiotic Aztreonarn to control gram-negative burn wound infection was considered to have
been achieved when the criteria of the effective topical agent were fulfilled, as
described above.
Aztreonam reduced the bacterial counts in a matter of days (4.0 ± 0.4), which is
significantly less than with essings. The reduced bacterial count was maintained for up to
21 days without superinfection, as shown by cultures.
Topical Aztreonam also controlled local and systemic manifestations of infection. However,
the presence of high fever necessitated the contemporaneous systemic administration of
Aztreonam.
In mixed secon ' d- and third-degree burns, micro-organisms are present within viable
tissue. Our study cast light on three issues:
The open burn wound has greater
absorptive power than normal skin. This explains the toxicity observed in early trials
with true antibiotics such as gentamicin, polymyxin, and sulphonamide, in which the
preparations had high concentrations, all originally with toxic effects in their
therapeutic dose. In our study we used a safe antibiotic without any toxic effect,"
and at a very low concentration estimated according to the MIC for all gram-negative
micro-organisms.
Burn wounds, especially in the presence
of Pseudomonas infection, are relatively ischaemic and the micro-organisms rarely
invade the blood. For this reason we applied the antibiotic topically, in order to ensure
adequate contact with the micro-organisms.
The p11 of burn wounds presenting
gram-negative infection usually ranges from 6.7 to 8.0,11 which allows the drug to be
active.
The idea of using antibiotics topically is
supported by the finding of Boucher et al .32 that the pharmacokinetics of antibiotics is
not the same in burned and nonburned patients. This necessitates dosage adjustment if the
antibiotic is to be used systemically.
The emergence of resistant organisms constitutes a problem that has to be faced with all
antimicrobial drugs, since it is difficult to reduce the bacterial count to zero per g of
tissue unless the wound is covered or healed. The routine use of one or two types of
topical agents has been associated with a high rate of resistant organisms, particularly
in settings with large numbers of patients and inadequate isolation facilities. A
repetition of this trial with other antibiotics would therefore widen the scope of topical
antimiocrobials used.
Conclusion
The idea of applying a true antibiotic
topically in order to control gram-negative burn wound infection was developed from our
use of a pretested agent against certain types of micro-organisms and a low-concentration
sensitivity test. We regard the present trial as a precursor to the use of other types of
antibiotics, provided they have a wide safety profile, are not irritant, are
water-soluble, and act at a pH similar to that of the micro-organisms.
The use of Aztreonam as a topical dressing is very helpful in the control of gram-negative
mixed second- and third-degree degree burn wound infections, in particular those due to Pseudomonas.
In the presence of high fever over 38.5 'C it is advisable to administer Aztreonam
also systemically.
RESUME. Les Auteurs se sont
occupés dans cette étude de 68 patients atteints de brûlures mixtes de deuxième et
troisième degré et/ou zones cruentées hospitalisés dans l'Unité des Brûlés et le
Centre des Brûlés de Assiut (Egypte) dans le but d'étudier l'effet de l'Aztreonam dans
le contrôle de l'infection des brûlures due aux bactéries à Gram négatif soit en
administrant l'antibiotique seulement en manière topique soit en association avec
l'administration systémique. Les résultats ont été comparés avec ceux d'un groupe
témoin composé de 57 patients atteints d'une infection de type Gram négatif qui ont
reçu une médication classique. Lévaluation a été effectuée sur des bases clinique et
bactériologique. Les Auteurs concluent que l'emploi de l'Aztreonam comme médication
topique se révèle très utile dans la lutte contre les infections de type Gram négatif
des brûlures mixtes de deuxième et troisième degré, et en particulier les
manifestations dues à Pseudornonas. Si le patient présente une forte fièvre
supérieure à 38,5 'C les Auteurs recommandent l'emploi aussi systémique de l'Aztreonam.
BIBLIOGRAPHY
- Papim R.P., Wilson A.P. et al.: Wound management in burn
centres in the United Kingdom. Br. J. Surg., 82: 505-9, 1995.
- Kamal M.S. et al.: Kasar El-Aim Burn Centre, Egypt. A
bacteriologic survey. Egypt J. Plast. Reconstr. Surg., 1979.
- Weber J.M., Tompkins O.M.: Improving survival: infection
control and burns. AACN Clin. Issues Crit. Care Nurs., 4: 414-23, 1993.
- Donati L., Scamazzo F, Fervasom M. et al.: Infection and
antibiotic therapy in 4000 burned patients treated in Milan, Italy, between 1976 and 1988.
Burns, 19: 345-8, 1993.
- Tredget E.E., Shankowsky H.A., Joffe A.M. et al.:
Epidemiology of infections with Pseudomonas aeruginosa in burn patients. The role
Il.of hydrotherapy. Clin. Inf. Dis., 15: 941-9, 1992
- Zhang Y.P.: Common pathogens in burn infection and changes
in their drug sensitivity. Chung-Cheng-Hsing-Shao-Shang-Wai-Ko-Tsa (Chin.), 7: 108-10,
157-9, 1991.
- Robert J.S.: Management of infection in the burn patient.
In: "Manual of Burn Therapeutics", Little Brown and Co., Boston, 1983.
- Wu SX, Liu YX: Molecular epiderniologic study of burn wound
infection caused by Staphylococcus aureas in children. Chin. Med. J. (Engl)., 107:
570-3, 1994.
- Basak S., Dutta S.U., Gupta S., Ganguly A.C., De R.:
Bacteriology of wound infection, evaluation by surface swab, and quantitative
full-thickness wound biopsy culture. J. Indian Med. Assoc., 90: 334. 1992.
- Robson M.C.: Burn Sepsis. Crit. Care Clin. North Am., 4:
281, 1988.
- Teplitz C. et al.: Pseudomonas burn wound sepsis. I.
Pathogenesis of experimental Pseudomonas burn wound sepsis. J. Surg. Res., 4: 200,
1964.
- Walker ILL., Mason A.D., Raulston G.L.: Surface infection
with Pseudomonas aeruginosa. Ann. Surg., 160: 297, 1964.
- Order S.E., Mancrif J.A.: "The burn wound",
Charles C. Thomas, Springfield, 1965.
- Dodd-Dend Stutman H.R.: Current issues in burn wound
infections. Adv. Pediatr. Infect. Dis., 6: 137-62, 1991.
- Grayson L.S., Hansbrough J.F., Zapata-Sirvent R.L. et al.:
Pharmacokinetics of Depofoam gentamicin delivery system and effect on soft tissue
infection. J. Surg. Res., 55: 559-64, 1993.
- Ross D.D., Phipps A.J., Clarke J.A.: The use of cerium
nitrate-silver sulphadiazine as a topical burns dressing. Br. J. Plast. Surg., 46: 582-4,
1993.
- William W.M., Bruce F.: Topical therapy for Burns. Surg.
Clin. North America, 67: 1987.
- Deitch E.A., Winterton J., Berg R.: Thermal injury promotes
bacterial translocation from the gastrointestinal tract in mice with impaired T-cell
mediated immunity. Arch. Surg., 121: 97-101, 1986.
- Yurt R.W., McManus A.T., Mason A.D., Jr. et al.: Increased
susceptibility in infection related to extent of burn injury. Arch. Surg., 119: 183-8,
1984.
- Touroutsoglou W., Sion M.L., Stathopoulos G. et al.:
Comparative study of Aztreonarn and cefamandole in the treatment of serious urinary tract
infection. Meth. Find. Expt. Clin. Phannacol., 5: 385-90, 1983.
- Bonner D.P., Sykes R.B.: Aztreonam: development and
antibacterial properties. Cherniot., 4 (Suppl.): 5-13, 1985.
- Sykes R.B., Bonner D.P., Bush K. et al.: Aztreonam (SQ 26,
776), a synthetic monobactam specifically active against aerobic gramnegative bacteria.
Antimicrob. Agents Chemother., 21: 85-92, 1982.
- Hall L.M., Livermore D.M., Gur D. et al.: OXA- 11, an
extendedspectrum variant of OAA-10 (PSE-2) beta lactamase from Pseudomonas aeruginosa. Antimicrob.
Agents Chemother., 37: 1637-44,1993.
- Bodey G.P., Tadeja L., Swabb E.A. et al.: Pharmacokinetic
studies ofAztreonam. In: Program and Abstracts of the 23rd Interscience Conference on
Antimicrobial Agents and Chemotherapy, Washington DC (Am, Sec. Microbiol.), Abstracts 411,
1983.
- Bonina L., Leonardi M.S., Delfino D. et al.: Human
neutrophil granulocytes and rate of peritoneal macrophage function activity of Aztreonarn
and its possible immunogenicity. Proceedings of 13th International Congress of
Chemotherapy, Vienna, 1983.
- Hilling. Fourth International Symposium on Rapid Methods
and Automation in Microbiology and Immunology, Berlin, 1984.
- Atkinson ME, Jr., Swabb E.A., Surgerman A.A.: Immunology of
the monobactam Aztreonam. Antumcrob. Agents Chemother., 25: 93-7, 1984.
- Drug evaluation monographs. Topic: Aztreonam. Micromedex
Inc. 89: 1974-96.
- Brentano L., Moyer C.A., Gravens D.L., Monafa W.W.:
Bacteriology of large human burns treated with silver nitrate. Arch. Surg., 93: 456-66,
1966.
- Georgiade N.G., Lucas M.C., Osterhout S.: A comparison of
methods for the quantitation of bacteria in burn wounds: clinical evaluation. Am. J. Clin.
Path., 53: 40-2, 1970.
- Chai J.K.: The pH value of granulating wound and skin graft
in burn patients. Chung- Hu a-Cheng - Hsing - Shao- Shang -Wai -Ko-Ts a (Chin.), 8: 177-8,
246, 1992.
- Boucher B.A., Kuhl D.A., Hickerson W.L.: Pharmacokinetics
of systemically administered antibiotics in patients with thermal injury. Clinic. Infect.
Dis., 14: 458-63, 1992.
- Zhang H.: Sensitivity of Staphylococcus aureus and Pseudomonas
aeruginosa and clinical application of antibiotics in patients with burn septicemia.
Chung-Hua-Wai-Ko-Tsa (Chin.), 30: 682-3, 700, 1992.
- Signorini M., Grappolim S., Magliano E. et al.: Updated
evaluation of the activity of antibiotics in burn centres. Burns, IS: 500-3, 1992.
- Clifford C.D., Arnold L., William C.P.: Systemic
antibiotics treatment in burned patients. Surg. Clin. North Am., 67: 1987.
- Overturf G.D., Zawacki B.E., Wilkins J.: Emergence of
resistance to amikacin during treatment of burn wounds: the role of antimicrobial
susceptibility testing. Surg. Arch., 79: 224, 1975.
This paper was
received on 22 January 1997.
Address correspondence to: Dr Assem
Hussain Kamel
Plastic and Reconstructive Surgery Unit, Assiut University Hospital
Assiut, Egypt.
Acknowledgement. The Authors
wish to thank Miss Jehan Abd El-Reheem,
Head Nurse, Burn Unit, Assiut University Hospital, Assiut for her fine efforts. |
|