| Annals of Burns and Fire Disasters - vol. X - n. 2
- June 1997
POST-BURN PATHOLOGICAL SCAR:
CLINICAL ASPECTS AND THERAPEUTIC APPROACH
Magliacani G.,(1) Stella M.,(1)
Castagnoli C.,(1) Trombotto (2) Ondei S.(2) Calcagni M.(1)
(1) Department of Plastic Surgery and
Burn Unit, Trauma Centre, Turin, Italy
(2) Centre for Immunogenetics and Experimental Oncology, National Research Council, Italy
SUMMARY. Pathological scarring continues to
represents a major challenge for reconstructive surgeons. its anatomopathological
classification is poorly defined and the relative epidemiological data are controversial.
Our research group has therefore drawn up a classification chart on the basis of the
morphological aspects of pathological scars. Hypertrophic scarring, the burn sequela most
frequently observed in our case records, is characterized by the onset of typical clinical
features which after a variable time course of activation undergo a phase of remission.
The factors that produce this progressive radical change in the scars are not clear. It
has recently been suggested that immunological factors may play a major role in the
pathogenesis of hypertrophic scars. In order to have a better understanding of the
pathophysiological factors involved, we studied active hypertrophic scars by means of
immunohistochemistry. Among the wide range of cytokines, only interferon y was highly
expressed in active hypertrophic scars on lymphocytes; it was less expressed in the
remission phase and in control samples. The management of abnormal wound response can be
considered appropriate only if it aims at the prevention or minimization of pathological
scarring, and the results can be considered satisfactory only if the therapy is successful
in specific anomalies related to particular lesions and in strict correlation with the
scarring evolution phase. It is therefore indispensable to adopt a common clinical
classification as this will provide better correlation between the clinical and the
biological situation and a better interpretation of the mechanisms responsible for
hypertrophic scarring.
Introduction
Pathological scarring still represents a major challenge for
reconstructive surgeons. This is due to many factors: poor knowledge of aetiopathogenesis,
the lack of a rational clinical classification, the absence of a scientific basis of
noninvasive therapy, and the limited results of treatment.
The importance of the management of pathological scars must not however be underestimated,
as they represent one of the most important limited factors for the complete recovery of
patients.
Even today, the diagnosis is based mainly on clinical judgement, since no laboratory test
is yet capable of evaluating the current state of a skin scar or of predicting its
evolution, healing time, and final outcome. Also, owing to the subjective nature of the
evaluation of lesions and to the lack of correlation between clinical status and
biological evolution, this type of diagnosis is not very reliable.
During its evolution, the scar structure undergoes continuous changes, particularly with
regard to its immunogenetic and histomorphological aspects, and even if a number of
histological, immunological, and biochemical studies have provided an abundance of new
evidence about the different aspects of pathological scarring, the real difficulty lies in
interrelating all the single elements to each other and to clinical findings.
The biological phase of the scar cannot be evaluated by any standard classification
criteria, as it is not correlated to the real evolutive state. This lack of classification
makes it impossible to conduct an accurate investigation of the various everchanging
aspects of pathological scarring. Scars have a poorly defined anatomopathological
classification, the epidemiological data are controversial, and the risk factors are
unknown.
Our experience has led us to believe that the first step towards a correct analysis and
understanding of this phenomenon is the collection of epidemiological data, and it is
therefore necessary to adopt a common clinical classification in order to permit, first of
all, a comparison of case reports.
On the basis of these considerations, we elaborated a classification chart according to
the morphological aspects of pathological scars, thus obtaining a better and more
homogeneous patient grouping. This takes into account: hypertrophy, hypertrophy and
contracture, contracture, and atrophy (Table 1).
| A. Hypertrophy |
generalized |
short |
| |
|
intermediate |
| |
limited |
long |
| B. Hypertrophy and contracture |
generalized |
short |
| |
|
intermediate |
| |
limited |
long |
| C. Contracture |
|
|
| D. Atrophy |
|
|
|
Table I - Clinical
classification of post-burn pathological scars |
|
Hypertrophy is the most frequently encountered pathology, either alone
or in combination with other pathologies, especially contracture, at the same time in the
same patient. Some biological aspects of hypertrophy are well known, such as continuous
collagen production, extracellular matrix abnormalities, in particular chondroitin
sulphate distribution, neovascularity, and increased cell turnover.
Clinically, the hypertrophic scar is a fibrous elevated skin lesion that normally does not
exceed the limits of the original injury, subsiding spontaneously after an initial
activation phase followed by a phase of regression. Initially it is erythematous,
elevated, painful, and pruritic, suggesting an inflammatory phenomenon. This phase may
persist for long periods of time and varies considerably from individual to individual.
The end of the activation phase is marked by a progressive decrease of the inflammatory
symptoms.
After months or even years, the scar flattens, softens, and blanches and there is a
reduction in dysaesthesia. These phases correspond to the various important modifications
in the tissues, particularly with regard to immunocompetent cell and cytokine production.
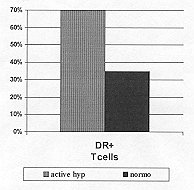
In active hypertrophic scars activated T cells represent 70% of leukocyte infiltrates,
compared with a maximum of 30% in normotrophic scars, where infiltrates are less abundant (Fig.
1). This suggests that immunocompetent cells play a pivotal role in the mechanisms
that lead to hypertrophy.
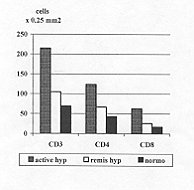
CD3, CD4, and CD8 T cells differ significantly in active hypertrophic scars when compared
with those observed in regressive hypertrophic scars and normotrophic scars (p >
0.0001) (Fig. 2). Lymphocytes infiltrate the deep and superficial dermis and are
also observed in the epidermis.
 |
 |
| Fig. I - Percentage of activated T
lymphocytes in post-burn scar tissues. |
Fig. 2 - CD3, CN, CD8 lymphocytes
per 0,25 MM2 in scar tissues. |
|
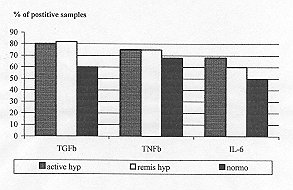
After activation, the T cells release several cytokines, intercellular
signals that show major changes as they pass from the active to the regressive phase. With
regard to the tumour necrosis factor B (TNF B), the transforming growth factor 8 (TGF B),
and interleukin6 (IL-6) positive samples, there are no significant differences in the
active and regressive phase of hypertrophic scars or in controls (Fig. 3).
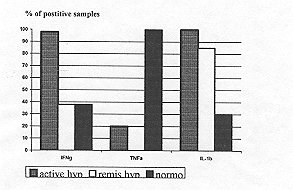
The number of positive specimens for interleukin-IB (ILAB) is significantly higher in all
hypertrophic scars than in normotrophic scars, while the percentage of positive samples
for turnout necrosis factor a (TNF (x) is significantly lower in active and regressive
hypertrophic scars than in controls.
Interferon 7 (IFNy) positivity is higher in active hipertrophic scars when compared with
the regressive phase and control (Fig. 4).
 |
 |
| Fig. 3 - TGFP, TNFP, IL-6 detection
in scar tissues |
Fig. 4 - IFN7, TNFu., IL- 10
detection in scar tissues |
|
It is evident that there are significant differences between the active
and the regressive phases of hypertrophic scars, while there are no differences between
the regressive phase of hypertrophy and normotrophic scars. The only changed cytokine in
the regressive phase is IFN y - which might well be considered a regression marker - and
this correlates well with the clinical evolution.
The onset time for the remission phase and the total duration of hypertrophy regression
are still controversial. According to the classification proposed by Muir in 1990,9 we can
consider three groups of scars: short-term evolution, when they are active for a maximum
period of six months and then remain static for some months, after which remission begins
and normally becomes complete in one year after healing; long-term evolution, when the
activity continues for years and the scar often spreads to the surrounding normal skin;
and an intermediate group, when they normalize within two years.
As to distribution, scars can he generalized (when they involve all areas of spontaneous
healing, grafting surfaces, or donor sites) or localized (when limited to some portions of
these areas (Table I).
In burn patients, the importance of the anatomical region remains to be clarified:
hypertrophic scarring in fact seems to be only partially associated with areas
traditionally considered more liable to hypertrophy than others.
When both hypertrophy and contracture are present, there is not only hypertrophy but also
skin coarctation, with a reduction in the surface area determined by centripetal forces of
variable strength, tending to evolve into atrophy and/or chronic ulceration and to
transform into neoplastic lesions.
On the basis of this classification, 293 patients were analysed: 21% were normotrophic,
34% were hypertrophic, 4% had contractures, 29% were hypertrophic with contractures, and
12% were not yet classifiable.
These data indicate that some kind of abnormal wound healing process was present in 67% of
burn patients: thus, even if pathological scarring is extremely frequent, it is not an
inevitable sequela.
The data also confirm our conviction that hypertrophy and contracture should be classified
separately if we are to have a better understanding of the pathophysiology of pathological
scarring.
With regard to distribution, 3 1 % of scars were generalized and 69% localized. Regarding
the time of evolution, the data show that 21.5% were short-term, 32.5% intermediate, and
46.0% long-term evolution scars.
As for the question of treatment, we shall limit our observations to noninvasive
management. There are - and always have been - many therapeutic trends but, to quote
Linares,' "with the same degree of confusion and controversy as their morphological
and etiopathogenic descriptions, owing to the fact that there is not enough scientific
demonstration of their effectiveness.
Several therapies have been proposed for hypertrophic scars, and this diversity reflects
the clinical heterogeneity of such lesions. They can be treated with physical methods,
such as Pressure devices, cryotherapy, and laser therapy, or with pharmacological methods,
such as topical therapy with retinoic acid and intralesional corticosteroid injection,
while recent preliminary reports have suggested that human recombinant interferon y exerts
a successful action.
Pressure by means of elastic garments and silicon gel sheeting or ordinary tapes are a
much~used and very easy method to obtain a thinning effect. The mechanism of this effect
is unknown: many hypotheses have been put forward but there is no general agreement.
A number of researchers have claimed varying degrees of success, often only slight, with
cryotherapy and laser therapy, which induce cell disruption. However, the subsequent
reshaping within the tissues has not been fully investigated. Good cosmetic results and
relief of symptoms have been obtained with radiation therapy. There are however in the
literature reports of neoplasms and radiation effects in body structures, even if recent
research has demonstrated that appropriate dosimetry and shielding can limit these adverse
effects.Topical retinoids have been reported to decrease fibroblast proliferation and to
reduce collagen synthesis in vitro, but their true action is unclear. No studies
have yet been performed in vivo. The intralesional corticosteroid response rate is
extremely variable and dosage and administration times are arbitrary. Also, steroid
deposition may lead to hypopigmentation, atrophy, telangectasis, and/or necrosis. Steroids
have been shown to produce a systemic response and cannot therefore be used safely in
generalized hypertrophy.
Our experience includes interesting observations of intralesional human interferon, which
shows different behaviours in the various scar evolution phases.
Our studies demonstrate that interferon y and its receptor are highly expressed in active
hypertrophic scars and start to decrease at the beginning of the regression phase (Fig.
3).
No trials reported in the literature explain the evolutive status and we must consider
whether the promising results are to be imputed to the drug used in the regressive phase,
when the interferon y rate is low, or to a dose-related effect, when the drug is used
during the active phase.
At present we are unable to answer this question, and further studies are needed to
establish interferon y's efficacy and to justify its cost compared with that of other
therapies.
It must also be considered that interferon, like steroids, has systemic effects and can be
used only in restricted scars and not in extensive scarring pathologies. In conclusion, it
is essential in our opinion to adopt a common clinical classification, as it has been
demonstrated that the morphology of each scar not only differs from patient to patient but
also in the same patient, in areas Of the same scar, and in the different evolutive
phases.
The purpose of the classification is to enable the clinician to make an accurate
identification of the kind and stage of the scar and to predict the clinical course of
abnormal healing. Current clinical classification criteria are unsatisfactory, as there is
no relationship between the clinical and the biological situation. This gives rise to an
excessive variety of aetiopathogenic interpretations of the mechanism responsible for
hypertrophic scarring. When every aspect of the pathogenesis of hypertrophy is better
understood, it will be possible to have a sound biological basis on which to plan more
effective prevention and treatment of pathological healing, with minimal complications.
The management of abnormal wound response can be considered appropriate only if it aims at
the prevention or minimization of pathological scarring, and the results can be considered
satisfactory only if the therapy is successful in specific anomalies related to particular
lesions and in strict correlation with the scarring evolution phase. Failing these
conditions, every attempt to formulate a rational treatment will be inadequate and even if
there may be numerous therapeutic proposals, the net result in most cases will be
frustration.
RESUME. La cicatrisation pathologique continue �
constituer un gros probl�me pour les chirurgiens reconstructifs, qui doivent se fier �
une classification anatomopathologique tr�s approximative et � des donn�es
�pid�miologiques controverses. Pour ces raisons notre groupe de recherche a pr�par� un
tableau de classification bas� sur les aspects morphologiques des cicatrices
pathologiques. La cicatrice hypertrophique, la s�quelle des br�lures la plus commune
dans notre casuistique, est caracteris�e par la manifestation de certaines
particularit�s cliniques typiques suivie, apr�s une p�riode variable d'activation, par
une phase de r�mission. Les facteurs qui provoquent cette transformation radicale des
cicatrices ne sont pas bien compris. R�cemment l'hypoth�s� a �t� formul�e que
certains facteurs immunologiques puissent jouer un r�le majeur dans la
pathogen�se des cicatrices hypertrophiques. Pour �tudier plus en profondeur ces aspects
pathophysiologiques, nous avons sommes servis de l'immunohistochimie pour �tudier les
cicatrices hypertrophiques actives. Nous avons examin� une large gamine de cytokines,
dont seulement l'interf�rony est hautement exprim� sur les lymphocytes des cicatrices
hypertrophiques actives; il est moins exprim� dans la phase de r�mission et dans les
t�moins. La gestion du d�veloppement anormal des l�sions peut �tre d�finie
appropri�e si elle mire � la pr�vention ou � la r�duction de la cicatrisation
pathologique, et les r�sultats peuvent se consid�rer satisfaisants seulement si la
th�rapie r�ussit dans le cas de certaines anomalies sp�cifiques li�es � des l�sions
particuli�res et en rigoureuse corr�lation avec la phase de l'�volution de la
cicatrisation. Il est donc essentiel d'adopter une classification clinique commune parce
qu'elle pourra nous donner une corr�lation meilleure entre la situation clinique et la
situation biologique et une interpr�tation meilleure des m�canismes responsables de la
cicatrisation hypertrophique.
BIBLIOGRAPHY
- Linares H.A.: From wound to scar. Burns, 22:
339-52, 1996.
- Bloch E.F., Hall M.G., Denson M.L et al.:
General immune reactivity in keloid patients. Plast. Reconstr. Surg., 73: 448-52, 1984.
- Castagnoli C., Stella M., Magliacani G. et al.:
Anomalous expression of HLA class 11 molecules on kerotinocytes and fibroblasts in
hypertrophic scars consequent to thermal injury. Clin. Exp. Immunol., 82: 350-4, 1990.
- Castagnoli C. , Stella M., Menegatti E. et al.:
CD36 expression in hypertrophic scars. Ann. Medit. Burns Club, 8: 214-8, 1995.
- Stella M., Castagnoli C., Magliacam G. et al.:
Fisiopatologia delta cicatrizzazione patologica (Revisione Bibliografica). Riv. Ital.
Chir. Plast., 21: 199-208, 1989.
- Magliacani G., Stella M., Ferrero R, et al.:
Epidemiology of pathological scarring in burnt patients. Abstracts, 9th ISB1 Congress,
473: 1994.
- Janssen de Limpens A.M.P., Cormane R.H.:
Studies on the immunologic aspects of keloid and hypertrophic scars. Arch. Dermat. Res.,
274: 259-64, 1982.
- Peacock E.E., Jr., Madden J.W., Trier W.C.:
Biological basis of treatment of keloid and hypertrophic scars. South Med. J., 63: 755,
1970.
- Muir I.F.K.: On the nature ol'keloid and
hypertrophic scars. Brit. J. Plast. Surg., 43: 61-9, 1990.
- Castagnoli C., Stella M., Berthed C. et al.:
TNF production in hypertrophic scarring. Cell Immunol., 147: 51-4, 1993.
- Kovacs E.J.: Fibrogenic cytokines: the role of
immune mediators in the development of scar tissue. Immunol. Today, 12: 17-23, 1991.
- Stella M., Castagnoli C., D'Alfonso S. et al.:
Cytokine expression in hypertrophic scarring. Abstracts, 9th ISBI Congress, 168: 1994.
- Castagnoli C., Stella M_ Magliacani M. et al.:
Similar ectopic expression of ICAM-1 and HLA Class 11 molecules in hypertrophic scars
following thermal injury. Burns, 20: 430-3, 1994.
- Castagnoli C., Stella M., Magliacani G. et al.:
The role ofTNF alpha and beta cytokines in scar hypertrophy in burn patients: an
immunohistochemical study. Anti. Medit. Burns Club, 8: 23-7, 1995.
- Peruccio D., Castagnoli C., Stella M. et al.:
Altered biosynthesis of TNF alpha is involved in post-burn hypertrophic scars. Burns, 20:
118-21, 1994.
- Castagnoli C., Trombotto C., Stella M. et al.:
Interferon gamma and interferon gamma receptor in post-burn hypertrophic scars: is it a
remission marker? Abstracts,VI Congress European Burns Association, 52: 1995.
- Murray J.C.: Scars and keloids. Dermat. Clin.,
ll: 697-708, 1993.
- Arturson G.: Pathophysiology of burn wound and
pharmacological treatment. Burns, 22: 255-74, 1996.
- Datubo-Brown D.: Keloids: A review of the
literature. Brit. J. Plast.Surg. 43: 70-7, 1990.
Acknowledgement. This work was supported by
the Piedmont Foundation for Burns Study and Research.This paper
was received on 25 February 1997.
Address correspondenee to: Dr Gilberto Magliacani,
Divisione di Chirurgia Plastica e Centro Ustioni, C.T.O.,
Via Zuretti 29, 10126 Torino, Italy (Tel.: 011.6933435;
Fax: 011.6933552). |
4th Congress of Pan-Arab
Association for Burns and
Plastic Surgery (PABPS) |
2nd Congress of Syrian Aesthetic
Reconstructive
Surgery and Burn Association (SARSBA) |
14 - 17 September
Aleppo-Syria
Topics: New Trends in Plastic and Aesthetic Surgery, Hand and Neck Surgery Reconstruction
of the Upper and Lower Extremity Burns Management and Prevention Disaster and Emergency
Medicine Congenital deformities
For information contact: Dr A. Dayoub - President PABPS
Aleppo, Syria
Tel.: 963-21 - 641501/2 - 218044 - 645710
Fax: 963-21 - 644900
P.O. Box: 6657
|
|
|