| Annals of Burns and Fire Disasters - vol. X - n. 2 - June 1997
RECONSTRUCTION
OF POST-BURN FACE DEFORMITIES
Gókalan L,(1) Ozgúr F.(2) Mavili E.,(2) Gúrsu
G.(2)
(1) Department of Plastic and Reconstructive Surgery,
Pamukkale University Faculty of Medicine, Denizli, Turkey
(2) Department of Plastic and Reconstructive Surgery, Hacettepe University Faculty
of Medicine, Ankara
SUMMARY. Over a 15-year period
(1978-1993), 123 procedures were used to reconstruct post-burn face deformities in 108 patients. Some of the
reconstructions were essential procedures, such as neck, microstomia and eyelid ectropion
release, by means of skin grafts, Zplastics, or local flaps. As these were the initial
steps of burned face repair, they were performed as early as possible, sometimes without
waiting for scar maturation. As an aesthetic procedure resurfacing of the face was
performed by dermabrasion and skin grafting. In some patients expanded skin flaps or free
flaps were used. Hair-bearing skin grafts or hair-bearing skin flaps pediculed by temporal
fascia were used for eyebrow reconstruction, local flaps or forehead flaps for nasal
reconstruction, and hair-bearing skin flaps from the temporoparietal region for moustache
reconstruction. Ear reconstruction was a difficult procedure, because of the poor quality
of the skin; the best results were obtained when the ear was reconstructed by costal
cartilage frames covered with temporal fascia and skin grafts.
Introduction
Facial burns represent between one-fourth and onethird of all burns. In a review conducted in a large burns unit
Dowling, Foley and Moncrief reported that nearly 60% of all patients admitted had facial
burns.' Among young children with burns, scald injuries caused by hot substances and flame
injury due to playing with matches are common! The groups most vulnerable to burn injury
are the very young, the elderly, and the physically handicapped. Although the causes of
burn injury are numerous, certain patterns appear in nearly every epidemiological study.
Flame burns due to the ignition of clothing, burns caused by flammable liquids bursting
into flame, and burns sustained in industrial accidents can all be severe and may involve
the face.
Plastic surgery procedures for burned face deformities are categorized as urgent
reconstructions, intermediate reconstructions, essential procedures, and late elective
reconstructions. Flap coverage of exposed bone or cartilage, a graft to protect an exposed
eye, or a release operation to allow the mouth to open for eating or for access for
anaesthesia or dental care are initial urgent steps in reconstruction and should be
performed in the acute phase. Neck release and lip or eyelid ectropion repair are
essential reconstructive procedures which should also be performed early. Reconstruction
of some parts of the face of aesthetic importance, e.g. resurfacing of the face,
reconstruction of eyebrows, lips, nose, and ear, as well as reconstruction of alopecic
parts of the scalp, are reconstructive procedures which can be performed electively, after
scar maturation?
This study was conducted in order to review the experience gained and the difficulties
encountered in the reconstruction of post-burn face deformities effected in Hacettepe
University Medical Faculty Department of Plastic and Reconstructive Surgery between 1978
and 1993.
Materials and methods
A retrospective survey was made of 123
reconstructive procedures for 108 post-burn face deformities performed since 1978 in the
clinic of Hacettepe University Faculty of Medicine Department of Plastic and
Reconstructive Surgery. All the patients had suffered severely deforming flame and
chemical burns in the face. All were attended with the aim of reconstruction, having
received their early treatment in a number of different clinics. None of the patients had
received any hypertrophic scar preventive therapy, such as the application of pressure
garments, silicone pads, splints, or inserts during the late phases of wound healing. The
reconstructive procedures were analysed in two different categories in relation to the
time of reconstruction, i.e. essential procedures and elective late procedures of burned
face reconstruction (Table I).
Essential
procedures
Neck release
Microstornia release
Eyelid ectropion release
Elective procedures
Resurfacing
Nasal reconstruction
Moustache reconstruction
Ear reconstruction
Eyebrow reconstruction |
25
7
21
19
14
3
21
24
|
|
Table
I - Types of reconstructive procedures for the face |
|
For neck release, Z-plasties and local
flaps were used to release scar bands, but in cases presenting severe skin defects, skin
grafts were the choice of reconstruction, followed by the use of collars (Table II)
(Cases 1,2).
| * Z-plasties and local flaps |
12 |
| * Skin grafts |
13 |
| Total |
25 |
|
|
Table II - Methods used for neck release |
|
As microstomia is an
important deformity which alters oral function, it is reconstructed as early as possible.
Such cases were released by local mucosal flaps as an initial step. Aesthetic repair of
the lips, nasolabial angle, and moustache was postponed to a later stage (Case 3).
Eyelid release was performed as an early reconstructive procedure for the restoration of
proper eyelid function, which is essential for the eye. The release of scar tissue by
means of skin grafts and the prevention of secondary contraction by tarsorrhaphy are the
usual procedures used for eyelids (Case 4).
For the resurfacing of the burned face good quality split-thickness skin grafts were
normally used in relation to the aesthetic units of the face. In some cases expanded skin
flaps and free flaps were also used to restore the face (Table III) (Cases 5,6,7).
* Skin grafts
* Expanded skin flaps
* Free flaps
* Expanded skin flaps and free flapsTotal |
11
5
2
1
19 |
|
Table
III - Methods used for resurfacing |
|
For nasal deformities, partial alar
defects were reconstructed by composite grafts and local flaps. For total nasal
reconstruction forehead flaps were used without hesitation, even if the forehead was
scarred (Table IV) (Case 8).
* Local flaps or composite grafts
* Forehead flaps Total |
9
5
14 |
|
Table
IV - Methods used for nasal reconstruction |
|
As partial defects of the ear can be
reconstructed by composite grafts or local flaps, the preferred method for total ear
reconstruction was a one-stage replacement of costal cartilage frames covered by temporal
fascia and skin grafts (Table V). A different procedure not among the classic
methods was adopted in a case of total ear loss in which superficial temporal fascia with
its overlying alopecic skin was used as a fasciocutaneous flap to cover the ear framework (Case
9).
* Local flaps or composite
grafts
* Costal cartilage flames covered by fasciaTotal |
12
9
21 |
|
Table
V - Methods used for ear reconstruction |
|
For moustache reconstruction in three
patients, a classic procedure was adopted in three patients, with hair-bearing skin flaps
used as island flaps based on the superficial temporal artery (Case 3).
For eyebrow reconstruction composite scalp grafts were the usual choice (Table VI) (Case
10).
• Scalp grafts
• Island scalp flapsTotal |
19
5
24 |
|
Table
VI - Methods used for eyebrow reconstruction |
|
Case reports
Case 1
A 12-year-old boy presented with a neck contracture five months after suffering scald
burns. The contracture was released and the skin defect was covered by splitthickness skin
grafts. The patient used a cervical collar post-operatively for six months (Fig. 1).
 |
 |
| Fig. la -
Case 1: Neck contraclure |
Fig. Ib
- Case 1: Released by skin graft. |
|
Case 2
A 10-year-old girl had a severely deforming skin contracture in the neck as a result
of scalds seven months before attending. The mandibular movements and mouth opening were
limited by the contracture. After release by skin graft the patient was advised to wear a
cervical collar for six months. However she abandoned the collar earlier than recommended
and the contracture partly recurred (Fig. 2).
 |
 |
| Fig. 2a
- Case 2: Neck contracture. |
Fig. 2b
- Case 2: Late result after 6 months. |
|
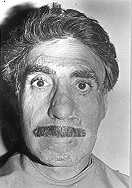
Case 3
A 24-year-old man was severely burned by phosphorus in an industrial accident. His
mouth and nostril openings were severely damaged. The microstomia and nostril rims were
released immediately and the patient used nostril retainers for six months. After the
essential problems had been solved moustache reconstruction with temporal island scalp
flaps was performed electively (Fig. 3).
 |
 |
| Fig.
3a - Case 3: Severely burned face with microstomia |
Fig.
3b - Case 3: A release of microstomia. |
|
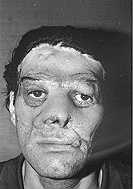
Case 4
A 47-year-old man presented with left eye ectropion as a result of burns seven months
before he attended. As an essential procedure the scar tissue on the left cheek was
released and reconstructed by means of a skin graft. Permanent tarsorrhaphy was used until
the skin graft took (Fig. 4).
 |
 |
| Fig. 4a
- Case 4: Ectropion of lower eyelid |
Fig. 4b
- Case 4: Late result after 8 months. |
|
Case 5
This 24-year-old woman had burn scars on the left side of the face which altered the
comer of the mouth. The deformity was electively reconstructed by an expanded skin flap
from the left mandibular region (Fig. 5).
 |
 |
 |
| Fig.
5a - Case 5: Irregular scars |
Fig.
5b - Case 5: Skin expanded.
on left of face |
Fig.
5c - Case 5: Late result
after 6 months. |
|
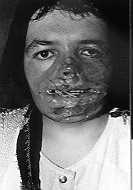
Case 6
This was a 21-year-old woman with severe flame burns. She was treated first with a
mouth splint and nostril retainers to prevent contraction of the mouth and nostril rims
during early care. Fourteen months later the lower lip and chin deformities were
reconstructed by means of an expanded skin flap from the neck. About two years later, the
left cheek and nasal dorsum were reconstructed by a free scapular skin flap (Fig. 6).
 |
 |
 |
Fig. 6a -
Case 6: Severe burn
deformity on left of face. |
Fig. 6b -
Case 6: Expanded skin
from neck used to replace the
scars in mandibular region |
Fig. 6c - Case
6: Nasal dorsum
and cheek reconstructed by
free scapular flap |
|
Case 7
A 27-year-old man who had been severely burned in childhood and subjected to several
reconstructive procedures attended in order to have his face resurfaced. The skin over the
nose and cheeks was replaced by free radial forearm flap (Fig. 7).
 |
 |
| Fig.
7a - Case 7: Severely deformed face. |
Fig.
7b - Case : dorsum of nose and bilateral cheeks reconstructed 5 months later. |
|
Case 8
This 34-year-old man had a severely deformed face as a result of chemical burns. The
eyelid defects were reconstructed by skin grafts. The nose was electively reconstructed by
a nasal hinge flap for the nostril rims and a forehead flap for the dorsum of the nose
(Fig. 8).
 |
 |
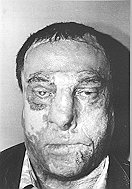 |
| Fig. 8a
- Case 8: Severely burned face. |
Fig. 8b -
Case 8: Lower part of nose reconstructed. |
Fig. 8c -
Case 8: Upper part
of nose reconstructed. |
|
Case 9
A 9-year-old girl suffered flame burns in the right side of the face and scalp five
years previously. The right car was completely lost and the right half of the scalp was
covered by a mesh graft when she attended. A 400 cc tissue expander was placed under the
scalp in the left parietal region in order to advance hair-bearing skin to the alopecic
region. As the expanded skin was advanced to replace the alopecic area, the ear was
reconstructed by a costal cartilage frame covered by the excised alopecic, matched grafted
skin as a flap pediculed by the superficial temporal artery. Although it was planned to
reconstruct the alopecic area on the occipital part of the head, the patient failed to
attend for further treatment (Fig. 9).
 |
 |
 |
| Fig.
9a - Case 9: Alopecia in right half of scalp with total ear loss. |
Fig.
9b - Case 9: Left parietal scalp expanded to restore alopecic right
parietotemporal region; this alopecie area was intended to be used as a flap based on the
superficial temporal fascia for eat reconstruction. |
Fig.
9c - Case 9: Left parietal scalp expanded to restore alopecic right
parictotemporal region; this alopecic area was intended to be used as a flap based on the
superficial temporal fascia for ear reconstruction. |
 |
|
 |
| Fig.
9d - Case 9: Ear reconstruction achieved by costal cartilage frame covered by
temporal fasciocutaneous flap. |
|
Fig.
9e - Case 9: Late result after one year. |
|
Case 10
This 10-year-old boy suffered flame burns in the face at the age of three. The
alopecic forehead scalp had been reconstructed by the advancement of hair-bearing scalp
from the back. The eyebrows were reconstructed by composite scalp grafts (Fig. 10).
 |
 |
| Fig. 10b - Case
10: Eyebrow reconstruction by complete scalp grafts. |
Fig. 10a - Case
10: Face burn as a result of flame. |
|
Results
Facial integrity was functionally
restored in all the patients by essential procedures such as neck, microstomia and eyelid
release. Neck contracture partly recurred in one case in this group as the patient showed
intolerance to collar usage (Case 2).
The results of elective procedures can be accepted as aesthetic improvements rather than
as complete restorations of the original. Resurfacing procedures had limited success
because of the difficulty of concealing the flap margin in expanded flaps and free skin
flaps (Cases 5 and 7). The loosening of free skin flaps was another unwelcome
result, giving the face a flaccid, bulky appearance (Case 7). Eyebrow and moustache
reconstructions by means of scalp flaps pediculed by a superficial temporal artery were
satis-factory - this was the most reliable method of hair-bearing skin flap transfer (Case
3). Eyebrow reconstruction by means of composite skin grafts resulted in partial hair
loss (Case 10). For ear reconstruction the best results were obtained by costal
cartilage frames covered by temporal fascia with skin grafts as a one-stage procedure (Case
9).
Discussion
Efforts to minimize the potential
disabling deformities of head and neck burns should be initiated during the acute period.
The priorities include the functional goals of the preservation of visual and oral
competence, the minimization of tissue loss, and the prevention of deforming chondritis
and neck contracture .4 Specific concerns during the acute phase are the prevention of
functional deformities such as eyelid ectropion and microstomia and the preservation of
the oral and nostril apertures. Early treatment of these problems may make later surgery
unnecessary. After healing of the wound and the use of splint inserts, pressure garments
and silicone pads for pressure therapy for the elimination of scars and the correction of
deformities, reconstructive procedures can be planned.Most of the patients in this study
who attended for reconstruction had received acute burn therapy in other clinics and they
presented severe deformities as a result of deficient therapy in the early phase of wound
healing.
Ideally, reconstructive efforts for improved appearance are delayed until a mature scar is
present. The length of time varies between six months and two years, and may even vary in
the same patient from one area to another. In the case of deformities affecting functional
goals such as neck contracture, microstomia and eyelid ectropion; early reconstruction is
necessary without waiting for scar maturation. These types of reconstructive procedures
can be regarded as essential procedures of post-burn face reconstruction.
In particular, eyelid deformities should be considered for early reconstruction in order
to prevent comeal ulceration and conjunctivitis. The release should be extensive, and
aesthetic units should be considered.' Conjunctival tarsorrhaphy is necessary for several
weeks until the graft takes. Tarsorraphy is not otherwise advised because of the deforming
effects on eyelid margins.
Neck contractures making intubation difficult and risky and other distorting facial
features necessitate early release and reconstruction. For moderate and mild deformities
band release by Z-plasties and local skin flaps are usually sufficient, but for severe
deformities such as cervicomental and mentosternal adhesions contracture release
necessitates tissue transfers such as skin grafts or free skin flaps. Flaps of bulky
appearance are not recommended if they deform the cervicomental angle.' For skin-grafted
necks, a period of six months of cervical collar usage is advised as otherwise contracture
may recur. The patient's compatibility is therefore important in this type of
reconstruction.
Other urgent procedures are microstomia release to allow the mouth to open for feeding and
breathing functions and for access for anaesthesia and dental care, as well as nostril
release for breathing functions. This can be achieved by adjacent mucosal flaps and skin
grafts. 10-14 To prevent secondary contracture, nostril retainers and mouth splints are
recommended to be used for at least six months.
Aesthetic restoration of the face for an acceptable normal appearance can be delayed until
the scars are mature. After a certain time the scars may become less prominent, thus
reducing the need for reconstructive procedures.
The resurfacing of the face by means of good quality skin grafts, paying special attention
to the different aesthetic units of the face, is the usual method of scar replacement for
the restoration of better appearance Staged reconstruction by means of neighbouring flaps
and tissue expansion of cervical skin with the subsequent advancement of burned neck skin
on to the face is another solution, but this type of reconstruction may limit neck
movement and lead to lower lid ectropion by creating tension. In larger areas free skin
flaps are recommended, although in some series they are criticized owing to their bulky
appearance.
For reconstruction of the nose, local flaps and skin grafts are advised, if they are
possible. In the case of severe deformities needing total nasal reconstruction,
forehead flaps or distant tissue transfers may be necessary.21 Forehead flaps are not
recommended as they create another scar on the face. 3,4 In the cases presented here,
nasal reconstruction was performed by means of flaps from the burn-scarred forehead, the
donor area being cover-ed by good quality skin graft. In this way forehead resurfacing was
achieved at the same time.
Partial car defects can easily be reconstructed by composite grafts' and local flaps such
as post-auricular tube flaps and conchal or helical chondrocutaneous flaps . For total ear
reconstruction all the classic techniques for microtia and traumatic ear deformities are
recommended. Total reconstruction of the burned ear is more difficult than other
deformities because of the poor quality of the skin.' In the cases presented here the best
results were obtained by a one-stage reconstruction by means of costal cartilage frames
covered by superficial temporal fascia with skin grafts. In alopecic scalps this technique
can be modified to a reconstruction with fasciocutaneous flaps for covering the costal
cartilage frames, as presented in one case.
Moustache and eyebrow reconstruction by island scalp flaps based on the superficial
temporal artery is a classic and reliable method. However, for eyebrow reconstruction,
these flaps are not always recommended because of the heavy hair density and the
side-effect of temporoparietal alopecia. Instead, composite scalp grafts can be used for
this process, although some hair follicles may be lost in the transfer process. To avoid
this problem, the technical details of harvesting scalp grafts were studied.
RESUME. Pendant une période
de 15 ans (1978-1993) les Auteurs ont effectué 123 procédures pour la reconstruction de
difformités du visages dues aux brûlures chez 108 patients. Certaines procédures
étaient essentielles, comme par exemple la libération du cou, de la microstomie, et de
l'ectropion palpébral, moyennant des greffes cutanées, des plasties en Z, et des
lambeaux locaux. Ces procédures de reconstruction, étant les premiers pas vers la
réparation du visage brûlé, ont été effectuées aussitôt que possible, même sans
attendre la maturation cicatricielle. Comme procédure aesthétique la surface du visage a
été recréée moyennant la dermabrasion et l'emploi de greffes cutanées. Dans certains
patients les Auteurs ont employé des lambeaux cutanés expansés ou des lambeaux libres.
Pour la reconstruction des sourcils ils ont utilisé des greffes cutanées pilifères ou
des lambeaux cutanés pilifères avec pédicule dans la fascia temporale, pour la
reconstruction du nez des lambeaux locaux ou des lambeaux du front, et pour la
reconstruction des moustaches des lambeaux cutanées pilifères de la région
temporopariétale. La reconstruction de l'oreille s'est révélée une procédure
difficile à cause de la qualité médiocre de la peau; les meilleurs résultats ont été
obtenus quand l'oreille a été reconstruite moyennant des structures cartilagineuses
costales couvertes par la fascia temporale et par des greffes cutanées.
BIBLIOGRAPHY
- Dowling J.A., Foley F.D., Moncrief JA.: Chondritis in the
burnedear. Plast. Reconstr. Surg., 42: 115, 1968.
- Feldman J.J.: Facial Burns. In: "Plastic
Surgery", McCarthy J.G. (Ed.), 2153-236, W.B. Saunders Co., Philadelphia, 1990
- Achauer B.M.: Reconstructing the burned face. Clin. Plast.
Surg., 19: 623-36, 1992.
- Achauer B.M.: Reconstruction of burn deformities of the
head and neck. In: "Mystery of Plastic and Reconstructive Surgery", Cohen M.,
Goldwyn R.M. (Eds.), 416-28, Little Brown and Co., Boston, New York, Toronto, London,
1994.
- Burns C.L., Chylack L.T., Jr: Thermal burns: the management
of thermal burns to the lids and globes. Ann. Ophtalmol., 11: 1358, 1979.
- Miller T.A.: Burns around eyes. In: "Burns: A team
approach", Artz C.T., Moncrief J.A., Pruitt B.A., It (Eds.), W.B. Saunders Co.,
Philadelphia, 1979.
- Jabaley M.E., Cat N.D., Lac N.T.: Use of local flap for
burn contracture of the neck. Plast. Reconstr. Surg., 79: 68, 1987.
- Spence R.J.: Clinical use of a tissue expander exchanged
transposition flap for face and neck reconstruction. Ann. Plast. Surg., 21: 58, 1988.
- Achauer B.M., Salibian A.H., Furnas D.W.: Free flaps to the
head and neck. Head and Neck Surg., 4: 315, 1982.
- Nath S., Erzingatsian K., Simond S.: Management of postburn
contracture of the neck. Burns, 20: 438-41, 1994.
- Smith L.K.: Correction of microstomia. Plast. Reconstr.
Surg., 14:302, 1954.
- Fairbanks G.R., Dingman R.O.: Restoration of the oral
commissure.Plast. Reconstr. Surg., 49: 411, 1972.
- Converse J.M.: Orbicularis advancement flap for
reconstruction of large angle mouth. Plast. Reconstr. Surg., 49: 99, 1972.
- Converse J.M. The over and out flap for restoration of the
comer of the mouth. Plast. Reconstr. Surg., 56: 575, 1975.
- Gonzales-Ulloa M.: Restoration of the face covering by
means of selected skin in regional aesthetic units. Br. J. Plast. Surg., 9: 212, 1956.
- Feldman J.J.: Reconstruction of the burned face in
children. In: "Pediatric Plastic Surgery", Serafin D., Georgiade N. (Eds.), 552,
C.V. Moby Co., St. Louis, 1984.
- Feldman J.J., Engraw L.H. et al.: Excision of burns of the
face.Plast. Reconstr. Surg., 77: 750, 1986.
- Argenta L.C., Vanderkolk C.A.: Tissue expansion in
craniofacial surgery. Clin. Plast. Surg., 14: 143, 1987.
- Schrudde J., Beinhoff U.: Reconstruction of the face by
means of the angle-rotation flaps. Aesth. Plast. Surg., It: 15, 1987.
- Gottlieb L.J., Parsons R.W., Krizek T.J.: The use of tissue
expansion techniques in burn reconstruction. J. Burn Care Rehabil., 7: 234, 1986.
- Elliott H.R.: Aesthetic restoration of severely disfigured
face in burn victims: A comprehensive strategy. Plast. Reconstr. Surg., 96: 157385, 1995,
- Juri J., Juri C., Belmont J.A., Grilli D.A., Angrigiani C.:
Neighbouring flaps and cartilage grafts for correction of serious nasal deformities.
Plast. Reconstr. Surg., 76: 876, 1985.
- Hauben D.J., Sagi A.: A sample method for alar rim
reconstruction. Plast. Reconstr. Surg., 80: 839, 1987.
- Spear S.L., Kroll S.S., Romm S.A.: A new twist to the
nasolabial flap for reconstruction of lateral alar defects. Plast. Reconstr. Surg.,
79:915,1987.
- Soeda S., Nakayama Y.: Nasal deformities due to burns.
Their surgical treatment. Burns, 6: 266-70, 1980.
- Antia N.H., Buch V.I.: Chondrocutaneous advancement flap
for the marginal defect of the ear. Plast. Reconstr. Surg., 39: 472, 1967.
- Goldstein JA., Stevenson T.R.: Reconstruction of the ear
helix: use of self-tubing pedicle flap. Ann. Plast. Surg., 21: 149, 1988.
- Donelan M.B.: Conchal transposition flap for postburn ear
deformities. Plast. Reconstr. Surg., 83: 641, 1989.
- Brent B.: Reconstruction of the ear, eyebrow and sideburn
in the burned patient. Plast. Reconstr. Surg., 55: 312, 1975.
- Tegtmeier R.I., Gooding R.A.: The use of fascial flap in
ear reconstruction. Plast. Reconstr. Surg., 60: 406-11, 1977.
- Pensler J.M., Dillon B., Parry S.W.: Reconstruction of the
eyebrow in the pediatric burned patient. Plast. Reconstr. Surg,, 76: 434-9, 1985.
Marks M.W., Friedman R.J., Thornton
J.W., Argenta L.C.: The ternporal island scalp flap for management of facial burn scars.
Plast. Reconstr. Surg., 82: 257-66, 1988.
This paper was
received on 6 May 1996.
Address correspondence to: Prof. Inci Gokalan
Pamukkale University Medical Faculty, Hastanesi, Doktorlar cad
20100 Denizli, Turkey
Fax: 0090 258 263 0827 |
|