| Annals of Burns and Fire Disasters - vol. X -
n. 2 - June 1997
EFFECTS OF HYPERTONIC SODIUM
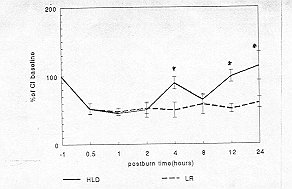
LACTATE DEXTRAN 70 RESUSCITATION ON CARDIAC FUNCTION IN SEVERELY BURNED DOGS SUMMARY. A comparative study was performed to evaluate the effects of resuscitation with hypertonic sodium lactate and dextran (HLD, Na+ 250 mmol/l sodium lactate with 6% dextran 70) and with lactated Ringer's solution (LR) on cardiac function, lipid peroxide level and heart tissue SOD activity. Dogs with 35% TBSA third-degree burns received I h post-burn either HLD resuscitation (19.6 inl/kg/3h; 14LD group, N' = 6) followed by LR 6 mllkgl% TBSA or LR resuscitation (10 ml/kg/% TBSA; LR group, N' = 6). The results ,Jiowed that the cardiac index was much higher in the HLD group than in the LR group 4, 8, 12 and 24 h post-burn. Cardiac contractility and relaxation were higher in the HLD group than in the LR group 12 and 24 h post-burn. The MDA level in heart tissue was much lower in the HLD group (17,41 Ý 2.82 mmol/g) than in the LR group (32.43 Ý 5.62 mmol/g) (p <0.01). Heart tissue SOD activity was much higher in the HLD group (157.49 Ý 32.23 p/g) than in the LR group (46.88 Ý 16.28 p/g) (p <0.01). These results suggest that HLD resuscita(ion may be beneficial in improving post-burn cardiac function and in attenuating post-burn oxidant-induced lipid peroxidation in the heart not only because of its oxygen-free radical scavenger but also because of its stimulation of heart tissue SOD activity. IntroductionThe resuscitation of circulatory shock with hypertonic solutions has been reported to restore systemic haemodynamics more effectively and more rapidly than isotonic solutions." In particular, hypertonic saline dextran 70 (HSD, 7.5% NaCl/6% dextran) has been used as a rapid expander of' intravascular volume in burn injury, proving to be beneficial in improving post-burn cardiac function. There are however some controversial issues in HSD resuscitation.In the present study, we compared the effects of hypertonic sodium lactate (Na+ 250 mmol/1) dextran 70 (HLD) Lind lactated Ringer's solution (LR) on post-burn cardiovascular function and lipid peroxidation of heart tissue. The cardiac function parameters included the cardiac index (CI), contractility (dp/dt max) and relaxation (-dp/dt max). We also investigated the level of MDA and SOD activity of heart tissue which presented lipid peroxidation indirectly. This plays an important role in post-burn injury. Methods Experimental design Operative preparation The study was performed in 12 healthy dogs weighing 10-15 kg. The animals were anaesthesized with intravenous injections of pentobarbital sodium (30 mg/kg). The back and flank skin of the animals was shaved to an area of 35% TBSA. An incision was made in the neck and a 2 turn catheter was inserted via the left common carotid artery into the left ventricle. A Swan-Ganz thermal dilution catheter (Model 93 a-131-7F, American Edwards Laboratories, Anasco, PR) was placed in the pulmonary artery through the left jugular vein. Measurement of cardiac function, MDA level and SOD activity The animals cardiac output (CO) was calculated by a cardiac output computer (Model 9520 cardiac output computer, American Edwards Laboratories, Anasco, PR), using the thermal dilutional method. Cl was calculated (CO/crn' body surface area), and dp/dt max and -dp/dt max were calculated by the CS-1 cardiac function computer (Second Military Medical University, Shanghai). MDA was measured according to the TBA-fluorometic method.' SOD activity was measured according to Chen et al.'s modified polarographic analysis method! The tissue protein level was measured by the Braford method! Braford agent was provided by the Biochemical Department of Fu Dan University, Shanghai. Statistical analysis The data, presented as the mean +SEM, were analysed as a two-factorial experiment with repeated measures. Comparative statistics of time effects were analysed using Dunnett's t test after ANOVA by comparing the values between time intervals to baseline values within each group. Between the groups, data at each time point were compared by using Student's unpaired t test. Statistical significance was accepted at p <0.05. Results Changes in CI
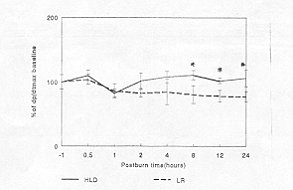
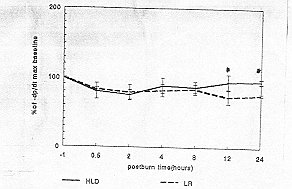
Changes in dpldt max and -dpldt max The dp/dt max and -dp/dt max in both groups increased slightly 0.5 h post-burn and then decreased I h post-burn. After resuscitation., the dp/dt max in the HLD group gradually resumed while in the LR group it did not. A significant difference between the two groups was noticed in the dp/dt max at 8, 12 and 24 h post-burn - it was much higher in the HLD group than in the LR group (p <0.01) (Fig. 2). The dp/dt max decreased 0.5 h post-burn in both groups: in the HLD group it dropped to 80.61 Ý 11.21% of baseline and in the LR group to 83.20 Ý 12.16% of baseline. After resuscitation, -dp/dt resumed slightly in both groups: in the HLD group it was much higher at 12 h (94.65 Ý 10.63% of baseline) and 24 h (95.70 Ý 3.44% of baseline) post-burn than in the LR group at 12 h (73.45 Ý 9.84% of baseline) and 24 h (76.45 Ý 1.62% of baseline) post-burn respectively (p <0.01) (Fig. 3).
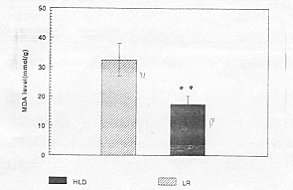
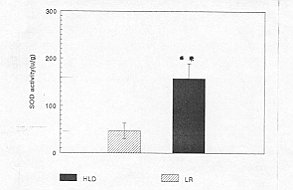
MDA levels and SOD activity in heart tissue NIDA levels in heart tissue were much lower in the HLD group (17.41 Ý 2.82 mmol/g) than in the LR group (32.34 Ý 5.62 mmol/g) (p <0.01). SOD activity in heart tissue was much higher in the HLD group (157.49 Ý 32.23 pg) than in the LR group (46.88 Ý 16.28 p/g) (p <0.01) (Figs. 4, 5).
Discussion HSD was used in burn resuscitation before the institution of crystalloid solution. Recent work by Onarheim et al.,' using an anaesthetized sheep model of thermal injury, showed that following thermal injury an HSD (4 ml/kg) bolus in 2 min improved cardiovascular function compared to an equal volume of 0.9% saline. These improvements were only transitory. We chose an infusion with 19.6 ml/kg HLD, which was more than the 10 ml/kg used by Tokyay et al.1 Our study showed that HLD resuscitation improved post-burn cardiac function parameters, including Cl, dp/dt max and -dp/dt max, better than LR resuscitation. This improvement lasted at least 12-24 h post-burn.Maningas et al.'o and Onarheim et al .4 showed that equal volumes of non-nal saline bolus infusion did not produce any significant improvement in cardiovascular function following shock. Our work showed that even LR resuscitation with a double dose of Parkland formula did not improve post-burn cardiac function. It is likely that physiological responses to the increased load of sodium and dextran caused the difference between the two groups. There is ample evidence in the literature that oxygenderived free radicals are produced after thermal injury, playing an important role in subsequent tissue darnage. Although the mechanism underlying the post-ischaemic injury is not completely understood and although oxidantinduced damage may encompass many cell components, peroxidative decomppsition of membrane lipids has been considered the basic cause of cell injury. 14 According to Tribble et al.11 lipid peroxidation is important in oxidative injury because it increases the number of free radical chain reactions, compromises detoxification systems, and causes direct deleterious effects. Tokyay et al.1 confirmed that HSD is beneficial in reducing the post-burn reperfusion injury seen with LR resuscitation, while Behrman et al.11 thought that reduced reperfusion injury with HSD resuscitation might be the result of dextran's oxygen free-radical scavenging and anti-neutrophil plugging properties. Our finding suggests that HLD could result in a decrease in the MDA level and an increase in SOD activity in heart tissue which might reduce the damage of lipid peroxidation to cardiac cell membrance. In conclusion, HLD resuscitation can improve postburn cardiac function, including Cl, dp/dt max and -dp/dt max, the improvement lasting for at least 12 h post-burn. Our findings suggest that hypertonic sodium lactate may be used in the early treatment of burns. RESUME. Les auteurs ont effectuÕ une Õtude comparative pour Õvaluer les effets de la rÕanimation avec le lactate de sodium hypertonique et dextran (HLD, Na+ 250 mmol/1 de lactate de sodium avec 6% dextran 70) et avec la solution lactatÕe de Ringer (LR) sur la fonction cardiaque, le niveau de peroxyde lipidique et l'activitÕ SOD du tissu cardiaque. Des chiens atteints de br«lures de troisiÒme degrÕ dans 35% de la surface totale corporelle (STC) ont reÓu 1 h aprÒs la br«lure ou la rÕanimation HLD (19,6 ml/kg/3h, groupe HLD, N' = 6) suivie par LR 6 ml/kg/% STC ou la rÕanimation LR (10 ml/kg/% STC; groupe LR, N' = 6). Les rÕsultats ont montrÕ que l'index cardiaque Õtait beaucoup plus ÕlevÕ dans le groupe HLD que dans le groupe LR 4, 8, 12 et 24 h aprÒs la br«lure. La contractilitÕ et la relaxation cardiaque Õtaient plus ÕlevÕes dans le groupe HLD que dans le groupe LR 12 et 24 h aprÒs la br«lure. Le niveau MDA du tissu cardiaque dans le groupe HLD (l 7,41 Ý 2,82 mmol/g) Õtait beaucoup plus bas que dans le groupe LR (32,43 Ý 5,62 mmol/g) (p <0,01). UactivitÕ SOD du tissu cardiaque dans le groupe HLD (157,49 Ý 12,23 p/g) Õtait beaucoup plus ÕlevÕe dans le groupe LR (46,88 Ý 16,28 p/g) (p <0,01). Ces rÕsultats indiquent que la rÕanimation des patients br«lÕs avec HLD peut õtre utile pour amÕliorer la fonction cardiaque et pour attÕnuer la peroxydation lipidique dans le coeur induite par l'oxy(tant non seulement Á cause de son macrophage radical sans oxygÒne mais aussi Á cause de sa stimulation de l'activitÕ SOD du tissu cardiaque. BIBLIOGRAPHY
|