Annals
of Burns and Fire Disasters - vol. X - n. 2 - June 1997
SKIN WOUND ZONE AFTER
CHEMICAL INJURY IN EXPERIMENTAL CONDITIONS
Troshev K, Markov D.
Department of
Burns and Plastic Surgery, Naval Hospital, Bulgarian Military Medical Academy, Varna,
Bulgaria
SUMMARY. There is
a significant similarity between wound zones after chemical injuries with NaOH, H2SO4, and
HCI and after burn trauma. The morphological differences are not significant either with
regard to experimental and control groups or to different causes. This is confirmed by
investigations we have conducted on other kinds of wounding. After chemical injury to the
skin nonspecific processes occur in the wound zone. There is no difference in their
character and dynamics from other skin injuries. Some different metabolic processes may
take place, but these were not investigated in the present study. The same diagnostic and
therapeutic problems and possibilities exist after chemical injuries as after other kinds
of burns.
Introduction
Chemical burns are burns of a special kind, but while there are many research works on
electrotrauma few deal with chemical injuries. This is surprising, as there are many
skin-destroying substances, such as heavy metals, acids, bases, and salts.
The degree of injury depends on the chemical activity of the substance. We may suppose
that the active substance which damages different tissue cells in the wound zone is the
same as in all other kinds of skin trauma, although the destructive agents may be
different. There are some classic wound descriptions in the literature, but we have no
significant data on the wound zone following chemical injury. These circumstances led to
the present investigation, the aim of which was to study the morphological changes in the
wound zone after chemical trauma.
Materials and methods
The investigation was conducted using 105
Wistar rats (average weight 200 gm). After ether narcosis on a depilated back skin zone of
15 sq cm we used a cotton wad to apply a chemical substance consisting of a 50% solution
of HCI, H2SO4 or NaOH for 15 minutes. The wound zone was washed for 15 minutes under water
and then dried. Histological preparations were taken after the rats died under narcosis.
We used our current laboratory methodics for microscope investigations at the 6th hour and
on days 1, 3, 7, 14, 21, and 28. The preparation material always contained part of the
necrotic zone and a zone at a distance of 1 cm. The rats were distributed in experimental groups of five animals
each. During the experimental period the animals lived in individual cages under standard
conditions. As a control group we used the results from the same methods of investigation
of the wound zone of skin after nonchemical trauma.
Results
Clinical observations.
Because of the lack of any specific methodology for experimental chemical skin wounds, we
were obliged to conduct a preliminary experiment by creating wounds with 100% solutions of
HCI, H2S04 or NaOH. After the experiment there was an immediate widening of the zone of
about 50%. The difference between the primary and the secondary wound area in the process
zone was established on the basis of different skin colours. Independently of water
washing, the animals were adynarnic, refused food, and died in the following one or two
days. We interpreted this as a result of intoxication and we applied 50% solutions.
 |
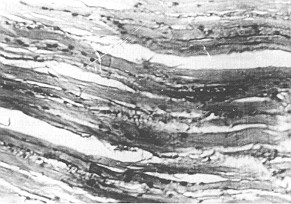 |
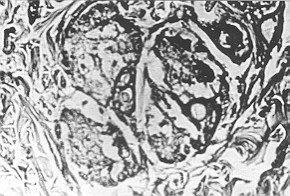
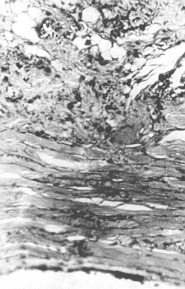
Fig. 1 - NaOH.
Gravely dystrophic and necrobiotic changes in all tissue cels in the epidermic and dermal
layers |
Fig. 2 - H2SO4.
Distrophic changes in epidermal layer and granular formations, wavy line of collagenous
fascicles, hyperaemia |
|
6 hr post-trauma.
There was fragmentation of the fibrillated structures and an increase in the number of
mast cells. The level of glycogen in the epidermal and muscle cells decreased. There was
haemodynamic collapse when the destroyed tissues enlarged. 24 hr post-trauma. Decrease of
haemostasis and gradual non-nalization of capillary lumen. No change in vessels with
erythrocyte thrombosis, aggravation of interstitial changes, serious oedema, small
cavitations in some cells. Myolysis in some muscle fibres. The keratin is detached from
the epidermal and dermal layers. The dystrophic changes in the superficial layers of the
epidermal stratum showed necrosis. Germinative layers cells remained cornparatively
preserved.
 |
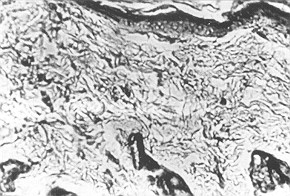
Fig. 3 - NaOH. In addition to the
main changes at the 6th hour there is also epidermial inflammation. There are many
macrophages among the inflamed cells. |
|
Day 3 post-trauma.
Autolysis of dead cells and structures in the epidermal and dermal layers. Inflammation
persisted. The number of leucocytes and macrophages increased, and no erythrocyte
thrombosis could be seen. The inflammatory reaction spread over the wound zone and the
superficial muscle layer. Moderate signs of regeneration of the epidermal cells and hair
follicles could be seen. NaOH. We can see epidermal necrosis and homogenization of the
dermal tissues and inflammatory subdermal infiltrates.
|
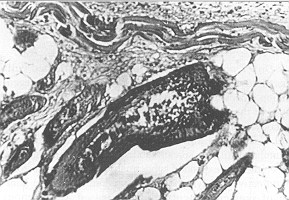
Fig. 4 - H2SO4. Dystrpphic and
necrobiotic changes in the cells. Inflammation and subdermal oedema. Inflammation
infiltrates of histiocyte and macrophage character. |
|
Day 7 post-trauma.
The number of inflamed cells decreased. Hyperaen-lia disappeared and significant
regeneration processes could be observed, especially at the basic layer in the epidermis
and hair follicles. The number of leucocytes and fibrocytes in the dermal layer increased,
and histiocytes and fibroblasts could also be seen. Granulation tissues spread subdermally
and the regenerated epithelium expanded subdermally to the necrotic zone. Germinative and
lymphoid cells predominated. The number of segmented neutrophils decreased. Collagenous
fibres precipitated and homogenized.

|
Fig. 5 - H2SO4. Dystrophic
changes, inflammatory oedema and inflamed cells can be seen. |
|
Day 14 post-trauma.
Complete regeneration of cover epithelium in the necrotic zone and differentiation of all
the cell layers. The process in the hair follicles was slower, while in the sebaceous and
sweat glands it was still starting. The homogenization and fragmentation of collagenous
fibres in the dermal layer state was unchanged. In the granulation tissue there was an
increase in the number of fibroblasts and fibrocytes, and a decrease in the number of
capillary vessels. Precollagenous and collagenous filaments appeared and inflammation was
still active in the deep layers, mainly presented by lymphoid cells and plasmocytes,
macrophages, and histiocytes.
|
Fig. 6 - NaOH. Initial
proliferation of young granulated tissues. |
|
Day 21 post-trauma.
NaOH. The covering of epithelium proliferated at the wound edge. In the superficial
necrotic layer there was precipitated calcium. There was also considerable proliferation
of fibroblasts and fibrocytes with fibroaenesis and young blood vessels. HS04. The
regeneration process was strengthened.hillammation in the granulated tissue was moderate.
HCI. No differences from H2SO4
|
Fig. 7 - NaOH. Granulation
tissue with expressed fibrogenesis under the scar |
|
Day 28 post-trauma.
There was no scar on the wound surface. In all tissues there were proliferation,
differentiation, and maturation. H2SO4. The wound was covered with fibrin. There was great
proliferation at the edge of the wound epithelium. Granulation in the bed of the wound and
regeneration processes in the skin adnexa were observed.HCl. No differences from H2SO4
group.
BIBLIOGRAPHY.
- Shindarski B.: Chemical burns. In
"Burntrauma", Medical Academy, Sofia, 1989.
- Simko S.: "Osetrovanie
popalenych", Osveta, Martin, 1985.
This
paper was received on 6 June 1994.
Address correspondence to: Prof. Konstantin Troshev, M.D., Ph.D
44 Alexander Batenberg Str.
9000 Varna, Bulgaria. |
G. WHITAKER INTERNATIONAL BURNS PRIZE
PALERMO, ITALY
Under the patronage of the Authorities of the Sicilian Region for 1998
By law n. 57 of June 14th 1983 the
Sicilian Regional Assembly authorized the President of the Region to grant the Giuseppe
Whitaker Foundation, a non-profit-making organization under the patronage of the Accademia
dei Lincei with seat in Palermo, an annual contribution for the establishment of the G.
Whitaker International Burns Prize aimed at recognizing the activity of the most qualified
experts from all countries in the field of burns pathology and treatment. The amount of
the prize is fixed at twenty million Italian Lire. The prize will be awarded every year by
the month of June in Palermo at the seat of the G. Whitaker Foundation.
The Adjudicating Committee is composed of the President of the Foundation, the President
of the Sicilian Region, the Representative of the Accadernia dei Lincei within the G.
Whitaker Foundation, the Dean of the Faculty of Medicine and Surgery of Palermo
University, the President of the Italian Society of Plastic Surgery, three experts in the
field of prevention, pathology, therapy and functional recovery of burns, the winner of
the prize awarded in the previous year, and a legal expert nominated in agreement with the
President of the Region as a guarantee of the respect for the scientific purpose which the
legislators intended to achieve when establishing the prize.
Anyone who considers himself/herself to be qualified to compete for the award may send by
January 31st 1998 a detailed curriculum vitae to: Michele Masellis M.D., Secretary-Member
of the Scientific Committee G. Whitaker Foundation, Via Dante 167, 90141 Palermo, Italy. |
|