Annals
of Burns and Fire Disasters - vol. X - n. 2 - June 1997
FLAMAZINE CREAM IN BURNS
Hadjiíski 0.,
Lesseva M., Tzolova N.
Centre for Burns and
Plastic Surgery, Pirogov Medical Institute, Sofia, Bulgaria
SUMMARY. Silver
sulphadiazine, used for the first time by Fox in 1968, is now the drug of choice for local
treatment of burn wounds, and Flamazine, its most popular compound, meets most of the
criteria for the ideal local agent. The aim of this study was to establish the efficacy of
Flamazine in the prevention of bacterial infection and in burn treatment. The study
concerned 50 hospitalized patients of either sex, aged between 1 and 76 years, with
second- and third-degree burns in 5 to 70% T13SA. The bacteriological results of Flamazine
application in 35 patients are presented. Both the open and the closed methods were used
for Flamazine application. All the patients were treafed successfully. In deep burns the
eschars were soft, slightly moist, metal grey in colour, and with no inflammation area in
or around them or any bacterial growth, this making it possible to perform early surgical
necrectomy. A good process of epithclialization initiated after debridement of superficial
burns. In 27 patients (77.0%) the wounds remained without bacterial growth from the time
of the patients' admission until they were operated on or until epithelialization. The
bacteriological results were evaluated as very good in 31 cases (88.5%) and good in four
(11.5%), with no unsatisfactory result. It is concluded that local treatment with
Flamazine is very important for the favourable course and outcome of the burn disease as
it prepares deep burns for early operative treatment and promotes rapid epithelialization
of superficial burns.
Introduction
Burn wound infection is the main source of
bacteraemia and an important cause of graft failure, which determines the essential role
of the agents for local antibacterial trteatment. 1,2 Unlike systemic antibiotics, local
agents penetrate burn wound surfaces with direct bacteriostatic and bactericidal action,
without damaging the tissues .2,3 Silver sulphadiazine, used for the first time by Fox in
1968, is now the drug of choice for the local treatment of burn wounds.
Flammazine consists of 10 mg per gram
micronized silver sulphadiazine in a hydrophilic cream base. This concentration provides
delivery of the agent in quantities above those necessary for in vitro inhibition of the
growth of susceptible micro-organisms. Silver sulphadiazine is highly effective in vitro
against gram-positive and gramnegative bacteria and fungi, including the common pathogens
found in burns (Table 1).
| Bacterial species Staphylococcus aureus
Coagulase-negative staphylococci
Streptococcus heta-haeniolyticus
Enterococcus
Pseudomonas aeruginosa
Klebsiella sp.
Enterobacter sp.
Serratia sp.
Proteus mirabilis
Proteus indol, (+)
Escherichia coli
Citrobacter sp.
Clostridiuni perfringens
Candida albicans |
Rates in%* 32.8
5.1
8.5
1.6
24.7
3.1
2.9
1.3
6.6
1.2
2.2
1.4
-
- |
MIC** (mkg/ml) 100
50
12.5
100
50
100
50-100
100
50
1.56-50
50
50
100
100 |
* Rates of the bacterial species in burn wounds infections
** MIC = Minimal inhibitory concentrations |
|
Table
I - Minimal inhibitorv concentrations of Flamazine against the most frequent
pathogem in burns |
|
The efficacy of Flamazine
is due to the combination of the bacteriostatic effect of sulphadiazine with the
bactericidal effect of silver. Clinical trials in large and small second- and third-degree
burns degrees have demonstrated the high antibacterial activity of Flamazine, which
delayed wound colonization in large burns until 10-14 days post-burn. These features
indicate that Flamazine possesses most of the criteria necessary for the ideal local agent
(Table 2).
Many publications proving the efficacy of Flamazine have appeared, but none concerning
investigations conducted in Bulgaria. There are however some reports on the use of other
silver sulphadiazine compounds (e.g. Dermazine) in our country.
The aim of this study was to assess the efficacy of Flamazine in the prevention of
bacterial infection and in burn treatment.
Requirements
of the ideal topical agent |
Features of
Flamazine |
| High
activity against gram-positive negative bacteria, fungi and viruses (lack of bacterial
resistance) Fasy to apply and
remove
Prolonged action
Good penetration into wounds and and eschars
Painless application; desirable analgesic effect
No adverse effect
No disturbance of epithelialization process
No discolouration of wounds
Not very expensive |
High activity
against and gramgram-positive and gram-negative bacteria, fungi and viruses (bacterial
resistance rare) Easy to apply
and remove
Possibility of residual effect
Good penetration into wounds; not deep enough
into eschars
Painless application; analgesic effect
Few, mild and transient adverse effects. No
effect on serum electrolytes or acid balance of blood; possibility of prolonged use
No disturbance of epithelialization process
Discolouration of wounds
Relatively expensive |
|
Table
II - Requirements of the ideal topical agent and the corresponding features of
Flamazine |
|
Material and methods
We treated 50
hospitalized patients of either sex aged between I and 76 years, as well as 25
out-patients. The treatment lasted from 4 to 25 days. All the patients were hospitalized
within 24 hr post-burn. In the out-patient group, the total body surface area (TBSA)
burned was between I and 6% (second- and third-degree); in the inpatient group, TBSA
ranged from 5 to 70% (also secondand third-degree) Table III presents the
bacteriological results are reported of Flamazine application in 35 patients. The
following aspects were considered:
the spectrum of bacteria
before and after Flamazine application, at every change of dressing
the number of bacteria
in I g of tissue, with a significant value of 101 bacteria per gram (b/g) accepted as the
criterion for the development of local and systemic infection
After conventional
cleansing of the wounds, we used the following two methods for the application of
Flamazine.
| N° |
Before
treatment |
After treatment |
|
Bacterial species |
Bacterial numbers |
Bacterial species |
Bacterial numbers |
| 1 |
no growth |
0 |
no growth |
0 |
| 2 |
no growth |
0 |
no growth |
0 |
| 3 |
no growth |
0 |
no growth |
0 |
| 4 |
no growth |
0 |
no growth |
0 |
| 5 |
no growth |
0 |
no growth |
0 |
| 6 |
no growth |
0 |
no growth |
0 |
| 7 |
no growth |
0 |
no growth |
0 |
| 8 |
no growth |
0 |
no growth |
0 |
| 9 |
no growth |
0 |
no growth |
0 |
| 10 |
no growth |
0 |
no growth |
0 |
| 11 |
CNS |
<103 b/g |
P. aeruginosa + Acinetobacter
sp. |
6x104 b/g |
| 12 |
CNS |
<103 b/g |
S. aureus |
104 b/g |
| 13 |
no growth |
0 |
no growth |
0 |
| 14 |
no growth |
0 |
no growth |
0 |
| 15 |
no growth |
0 |
no growth |
0 |
| 16 |
S. aureus |
0 |
no growth |
0 |
| 17 |
no growth |
0 |
no growth |
0 |
| 18 |
no growth |
0 |
no growth |
0 |
| 19 |
Acinetobacter sp. |
2.5x104 b/g |
no growth |
0 |
| 20 |
no growth |
0 |
no growth |
0 |
| 21 |
CNS |
1.5x105 b/g |
no growth |
0 |
| 22 |
no growth |
0 |
no growth |
0 |
| 23 |
no growth |
0 |
no growth |
0 |
| 24 |
S. aureus |
104 b/g |
no growth |
0 |
| 25 |
no growth |
0 |
no growth |
0 |
| 26 |
no growth |
0 |
no growth |
0 |
| 27 |
no growth |
0 |
Serratia sp. |
<103 b/g |
| 28 |
Enterobacter sp. |
6.6x105 b/g |
Enterobacter sp. |
1.1x104 b/g |
| 29 |
no growth |
0 |
no growth |
0 |
| 30 |
no growth |
0 |
no growth |
0 |
| 31 |
no growth |
0 |
no growth |
0 |
| 32 |
no growth |
0 |
no growth |
0 |
| 33 |
no growth |
0 |
no growth |
0 |
| 34 |
no growth |
0 |
no growth |
0 |
| 35 |
no growth |
0 |
no growth |
0 |
CNS =
coagulase-negative staphylococci
b/g = bacteria per gram |
|
Table
III - Bacteriological results of Flamazine application in 35 patients with
second- and third-degree burns |
|
Closed method
Flamazine was applied in a layer 2-3 mm thick directly on the burn wound by applicator
or by hand in a sterile glove. It was then covered with dry sterile gauze. The burn wound
was sometimes covered after a preliminary spread also with Flamazine sterile gauze. When
the hands were burned, they were placed in a polythene bag or sterile latex gloves
containing Flamazine. In this way the movements of the hands are painless and their
observation is easy.
Open method
The open method is convenient for burns of the face and perineum. Flamazine was spread
over the burned surfaces, which were left uncovered. The contact of the agent with the
unburned skin was painless and safe. Dressings were changed in most cases every 24 hours
during the first 10 days post-burn, and every 24-48 hours thereafter. When necessary,
dressings were changed more frequently. With the open method of treatment the agent could be changed more often,
i.e. every 6-12 hours. The easiest and most painless way of removing Flamazine from the
wound surface was to wash it out with sterile solution or water.
Results
Clinical observations
All the patients were cured: the out-patients and thirtyone of the in-patients after
non-surgical treatment, and nineteen of the hospitalized patients after surgical
treatment. Sixteen of these nineteen patients underwent early surgical necrectomy between
days 3 and 6 post-burn, while the remaining three were operated on ten and more days after
the accident. Spontaneous epithelialization of superficial burns took place in the
generally accepted terms, in relation to the depth of the injury.
The maintenance of no or low-level bacterial
contarnination of the wounds and the prevention of inflammation allowed early operative
treatment and good epithelialization of the wounds.
According to our observations, the eschars in deep burns were soft, slightly moist, metal
grey in colour, and with no inflammation area in or around them or any bacterial growth,
this making it possible to perform early surgical necrectomy. When this was not done, the
separation of the eschars was performed gradually, layer by layer, until full removement,
without any sign of local infection.
With regard to superficial burns, after Flamazine application the wounds were covered with
a heavy purulent exudation, which gave the false impression of a worsening of the burns
appearance. The exudation was in fact sterile and simply the result of the wound exudation
mixing with the topical drug. It was easy to remove and there was no sign of any real
worsening of the wounds. Deep dermal burns were sometimes covered with a thin coating of
Flamazine, mixed with proteins, dissolved in the wound exudation. These coatings were
easily removed by scraping them away or cleaning up during subsequent medications. After
repeated application of Flamazine the burn surfaces became fresh, with no unpleasant smell
or any sign of infectious complications. This was due to inhibition of bacterial growth
and the wounds improved condition. As a result, a good process of epithelialization
initiated after debridement.
Microbiological results
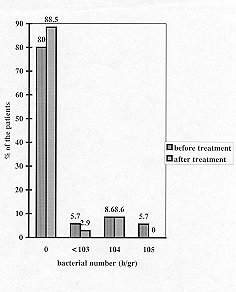
The bacteriological results in 35 patients are presented in Table 3 and Fig. 1. It
was established that:
- in 27 patients (77.0%) the wounds remained
without bacterial growth from the time of the patients' admission until the operation or
epithelalization of the wounds in 4 patients (N° 16, 19, 21, 24) (11.5%) the preexisting
bacteria were eradicated after Flamazine application, which means that the effect of the
agent was both therapeutic and prophylactic
in one patient (N° 28)
(2.9%) the bacterial quantity was reduced and after three medications (day 4) the
pre-existing bacterial pathogens were eradicated
in three patients (N°
11, 12, 27) (8.6%) bacterial colonization of the wounds occurred as follows: Pseudomonas
aeruginosa + Acinetobacter sp., days 3 to 5 (N° 11); Staphylococcus aureus, days
3 to 8 (N° 12); and Serratia sp., days 6 to 10 (N° 27). The bacterial quantities
in all three cases were below the significant value; no clinical signs for local or
systemic infection appeared, and the skin grafting and healing processes were not
disturbed
three patients developed
staphylococcal bacteraemia, due to Staphylococcus aureus in two patients and
coagulase-negative staphylococei in one. The origin in each case was contaminated central
venous can~ nulae; there were no cases of generalization of local infection (burn wound
sepsis)
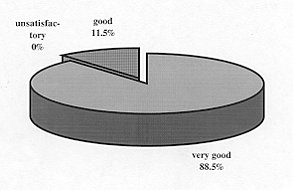
The results were evaluated as follows (Fig. 2):
No toxic reactions or
other side-effects were observed. The application of Flamazine was painless and
comfortahle for the patients.
 |
 |
| Fig.
1 - Bacteriological results of Flamazine treatment. |
Fig.
2 - Evaluation of treatment results. |
|
Conclusion
Our results demonstrate that Flamazine
exerts a prophylactic and therapeutic action against wound infection in burns, which was
proved both in vitro and in vivo. Considering that infection is the most
frequent and life-threatening complication in patients with severe burns, we consider that
local treatment with Flamazine is very important for the favourable course and outcome of
the burn disease as it prepares deep burns for early operative treatment and promotes
rapid epithelialization of superficial burns.
RESUME. La sulfadiazine
argentée, utilisée pour la premičre fois par Fox en 1968, est aujourd'hui le
médicament préféré pour le traitement local des brűlures, et Flarnazine, son composé
le plus diffus, répond ŕ la plupart des critčres de l'agent local idéal. Le but de
cette étude était d'établir l'efficacité de Flamazine dans la prévention de
l'infection bactérienne et dans le traitement des brűlures. Les Auteurs ont considéré
50 patients hospitalisés des deux sexes, âgés d'un an jusqu'ŕ 76, atteints de
brűlures de deuxičme et troisičme degré en 570% de la surface corporelle. Les Auteurs
présentent les résultats bactériologiques de l'application de Flamazine dans 35
patients. La Flamazine a été appliquée avec la méthode ou ouverte ou close. Tous les
patients ont été traités avec succčs. Dans les brűlures profondes les escarres
étaient molles, légčrement humides, de couleur gris métallique, et sans la présence
de zone d'inflammation ni de développement bactérien, ce qui permettait d'effectuer la
nécrectomie chirurgicale précoce. Un bon processus d'épithélialisation a commencé
aprčs le débridement des brűlures superficielles. Dans 27 patients (77,0%) les lésions
n'ont pas présenté aucun développement bactérien depuis le moment de l'hospitalisation
jusqu'ŕ l'opération chirurgicale ou l'épithélialisation. Les résultats
bactériologiques ont été évalués comme trčs bons dans 31 cas (88,5%) et bons dans
quatre (11,5%), sans aucun résultat peu satisfaisant. Les Auteurs concluent que le
traitement local avec Flamazine est trčs important pour le cours positif et le bon
résultat de la maladie des brűlés puisque ce médicament prépare les brűlures
profondes pour le traitement chirurgical précoce et favorise l'épithélialisation rapide
des brűlures superficielles.
BIBLIOGRAPHY
Fox C., Jr: Topical therapy and
the development of silver sulphadia zinc, Surg. Gynecol. Obstet., 157: 82-8, 1983.
Ge Sheng De, Hu Zheng Lu., Cheng In Lin et
al.: Experimental study on topical antimicrobial agents in burns. Burns, 13: 56-9,1987.
Gillett A.P.: Antibiotic prophylaxis and
therapy in burns. J. Hosp. it.Infect., 6 (Suppl. B), 59-66, 1985.
Fakhry S.N., Alexander J., Smith D., Meyer
A.A., Peterson H.D.:Regional and institutional variation in burn care. J. Burn Care
Rehabil., 16: 86-90, 1995.
Taddonio TE., Thomson P.D., Smith D.J.,
Prasad J.K.: A survey of wound monitoring and topical antimicrobial therapy practices in
the treatment of burn injury. J. Burn Care Rehabil., 11: 423-7, 1990.
Hermans R.P.,: Topical treatment of serious
infections with special reference to the use of rnixure of silver sulphadiazine and cerium
nitrate: two clinical studies. Burns, 11: 59-62, 1984.
Kuroyanagi J., Kim E., Shioya N.:
Evaluation of a synthetic wound dressing capable of releasing silver sulphadiazine. J.
Burn Care Rehabit. 12: 106-115, 1991.
Hoekstra MJ... Hupkens P., Dutrieux P. et
al.: A comparative burn wound model in the New Yorkshire pig for the histopathological
evaluation of local therapeutic regimens, silver sulphadiazine cream as a standard, Br. J.
Plast. Surg., 93, 46: 585-9.
Hoffmann S.: Silver sulphadiazine: an
antibacterial agent for topical use in burns. A review of the literature. Scand. J. Plast.
Reconstr. Surg., 18: 119-26, 1984.
Modak S., Fox P., Standford J. et al.:
Silver sulphadiazine impregnared biologic membranes as burn wound covers. J. Burn Care
Rehabil., 7: 422-5, 1986.
Sawhney C.P., Sharma R.K., Rao K.R.,
Kaushish R.: Long term experience with 1% topical silver sulphadiazine cream in the
management of burn wounds. Burns 15: 403-6, 1989.
Stem H.S.: Silver sulphadiazine and the
healing of partial thickness burns: a prospecctive clinical trial, Br. J. Plast. Surg.,
42: 581-5, 1989.
Schiller W.R., Leukens C., Neve D.:
The use of expanded polytetrafluoroethylene gloves for care of upper extremity burns. J.
Burn Care Rehabil., 15: 34-6, 1994.
This
paper was received on 7 November 1996.
Address correspondence to: Dr Ognian Hadjiiski,
Centre for Burns and Plastic Surgery, Pirogov Medical Institute,
21 Macedonia Blvd., 1605 Sofia, Bulgaria (Tel./Fax: 00359.2.546108) |
|