Annals
of Burns and Fire Disasters - vol. X - n. 3 - September 1997
THE STRATEGIC MANAGEMENT
OF THE HIGH-VOLTAGE ELECTRICAL INJURY
Cerepani M.J.,
Leonard L., Slater H., Goldfarb W.I.
The Western
Pennsylvania Hospital, Pittsburgh, Pa., USA
SUMMARY. The strategic
management of the high-voltage electrical injury can be both challenging and complex. The
challenge begins from the time of injury and continues through rehabilitation. The complex
aspect of management is the complications that occur due to systemic effects. A
35-year-old male sustained a 65% T13SA partial- and full-thickness electrical burns to the
lower extren~ties, posterior trunk, and occipital and parietal skull. He underwent sixteen
operations over a period of four months. The operations began with abovethe-knee
amputations of the bilateral lower extremities, multiple debridernent of hurried areas
with application of cadaver skin graft, splitthickness skin graft and placement of
cultured epidermal autograft, multiple debridement of open wound areas on the scalp, and a
colostomy. Throughout hospitalization many serious complications occurred. Some were
life-threatening and two remain unresolved. The lifethreatening setbacks included a long
course of vancomycin to treat MRSA (methycillin-resistant Staphylococcus aureus),
persistent diarrhoea, and inability to tolerate solid foods. The frequent surgeries
presented a problem for the patient's nutritional status, together with mobility concerns.
The unresolved problems remain an issue. A colostomy was performed early in the early
stage of hospitalization. It is unclear if it will be reversed. The patient developed
calcification of both shoulders, which has made movement extremely difficult. Although
these two problems have remained unresolved, the patient and his family consider them to
be a minor hurdle that they will conquen The challenge of this complex case of
high-voltage electrical injury will be one to remember for a lifetime.
S.S. was a 35-year-old man
who suffered extensive burns when he raised the bed of a truck that he was driving against
high-voltage electric lines. Witnesses stated that the patient was electrocuted as he
stepped from the truck to the ground. He was observed to be on the ground for several
minutes, after which he attempted to return to the truck, which then caught fire. He was
transferred to the Western Pennsylvania Hospital Burn Trauma Center and was found to have
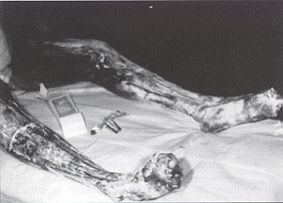
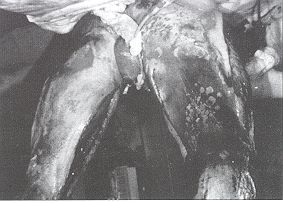
full-thickness burns on 65% of the body. The lower extremities from the mid-thighs
distally were coagulated with areas of exposed bone and open knee and ankle joints. The
entire posterior aspect of the body had a full-thickness burn extending deep into the
perineum and the perianal and periscrotal tissues (Figs. 1 and 2.) There was a
full-thickness burn on the occipital aspect of the skull which exposed the underlying
cranium. There were scattered burns on the anterior trunk, arms, and neck. At the time of
admission the patient was alert but had no memory of the accident. There was evidence of
myoglobinuria. After an initial assessment it was our impression that the patient had a
chance of surviving these terrible injuries and he expressed his willingness and desire
for full treatment as might be necessary to treat his injuries.
 |
 |
| Fig.
1 - Perineum. |
Fig.
2 - Perianal and periscrotal tissues. |
|
When one encounters
patients such as S.S., a long and complex hospital course may be anticipated. We feel that
it is of great importance to make a strategic plan that prioritizes and organizes the
patient's care. Specific early and late goals can be established and plans made to meet
the goals. We felt that the treatment of S.S. could be divided into sequential and
overlapping phases.
The first phase of S.S.'s treatment
involved resuscitation. He received a combination of lactated Ringer's solution and fresh
frozen plasma. The rate of fluid infusion was adjusted to obtain a urine output of I
ml/kg/h and regulated to promptly dilute the myoglobin in the patient's' urine. This was
accomplished with minimal weight gain. Despite deep burns about the head the patient did
not require ventilatory support. When resuscitation was initiated the patient underwent
fasciotornies on the lower extremities because of the deep nature of the burns. The
fasciotomies revealed that the patient had coagulated, nonviable muscle in all
compartments of the legs. He was placed on a cardiac monitor and a pulse oximeter and
responded well to resuscitation. Additional sequential plans for his management were then
devised.
We were of the opinion that the next phase of management involved debridement of nonviable
tissue. We did not feel we had total knowledge of the extent of full-thickness damage
early in the course of treatment. We also felt that we should limit blood loss and the
duration of debridement operations and it was therefore our plan to operate on the patient
early and return him to the operating room as necessary to complete the excision without
undue stress to the patient. S.S. had relatively few donor sites for skin grafts as
compared with the large area of his body that would require wound coverage. We anticipated
the need for cultured epithelial cells to augment widely meshed autograft and to cover
areas of the body where autograft was not available. We anticipated that the-patient would
need a temporary or permanent colostomy because of the severe burns around the perineum.
This operation would be timed to minimize the risk of sepsis secondary to faecal
contamination of his burns. The need for long-term nutritional support was anticipated and
plans were made to create a surgical jejunostomy so that early tube feeding could be
initiated and maintained through the patient's anticipated long hospitalization.
This strategic plan was discussed with the patient and his wife so that they would have a
sense of his overall management and of the magnitude of the problems to be faced in his
treatment. Both had a good understanding of the general outline of the plan and were
agreeable to its performance.
The patient responded well to resuscitation and was taken to the operating room on
hospital day 2, when bilateral above-the-knee amputations were performed. In order to
conserve as much femur and thigh length as possible, guillotine-type amputations were
done. Two full-thickness skin specimens 2 cm in diameter were harvested at the time of the
amputation. These were sent to Biosurface Technology Laboratories in Cambridge,
Massachusetts for cultured epithelial cell coverage. On hospital day 4 the patient
underwent a laparotomy in which a transverse loop colostomy was created and a catheter
jejunostomy created. S.S. continued to be stable and on hospital day 6 he was returned to
the operating room and his buttocks, perineum and posterior trunk, shoulders, neck, and
occipital scalp were debrided and cadaver skin grafts were placed.
Between hospital days 7 and 30, S.S. was repeatedly returned to the operating room.
Additional areas of nonviable tissue and nonadherent cadaver skin were excised and the
wounds covered with new cadaver skin. On hospital day 30, the cultured epithelial
autografts were flown to Pittsburgh and the patient's own skin was harvested in
ten-thousandths of an inch thick sheets which were meshed at a 4:1 ratio. These meshed
autograft sheets were placed on the patient's posterior trunk, neck, and shoulders.
Cultured epithelial cells were placed over the 4:1 meshed autograft and over
full-thickness wounds not covered with autograft. The patient was kept in a prone position
for the next ten days. Nutritional support with tube feedings via the catheter jejunostomy
was continued throughout this phase of treatment. The colostomy functioned well and there
was no perineal soiling. On hospital day 40, the posterior aspect of the patient's body
was undressed and we found an excellent take of the widely meshed autograft with complete
healing of the interstices that had been covered with cultured epithelial autograft (Fig.
3). A few days later the patient was turned from a prone to a supine position and kept on
an air flotation mattress.

|
Fig.
3 - Cultured epithelial autograft. |
|
A programme of
physical and occupational therapy was initiated a few days after admission. Various
range-ofmotion exercises were curtailed during the immediate post-skin-graft period for
fear of shearing the grafts. When the grafts were secure, range-of-motion exercises of the
upper extremities and femurs were re-instituted. In the days and weeks following hospital
day 40, S.S. was returned to the operating room on multiple occasions when fullthickness
skin grafts were placed over his occiput, and meshed autograft was placed over his revised
amputation stumps. On hospital day 130, S.S. was discharged to a rehabilitation institute.
The wounds were all closed and he no longer required jejunostomy feeding as his oral
intake was adequate. The patient had lost considerable range of motion of his shoulders
and was generally weak at the time of discharge.
S.S. was found to have heterotopic calcification around both shoulder joints. He had
regained some motion of the shoulders and was able to care for himself but could not
abduct the shoulders beyond 60 degrees bilaterally. He had a normal range of motion of his
elbows, wrists, and hands. Despite the deep perineal burns his sphincter function was
normal and he underwent closure of the colbstomy 12 weeks after discharge from the
hospital.
S.S. is continuing in a programme of intensive rehabilitation to attempt to increase the
range of motion of his shoulders. He has normal bowel function, is able to dress himself,
and is mobile with the use of a wheelchair. The patient and his wife are pleased with the
progress that he has made and are appreciative of the efforts made on his behalf.
We believe that this good outcome was obtained through strategic planning that considered
the patient's resuscitation, debridement, nutritional support, and wound coverage. Close
co-operation and co-ordination between the treatment team - composed of physicians,
nurses, nutritionists, and physical and occupational therapists - is important for a
favourable outcome in severely injured patients such as this one.
RESUME.
La gestion stratégique des lésions électriques causées par la haute tension est ŕ la
fois difficile et complexe. Les difficultés commencent dčs le moment de la lésion et
continuent jusqu'ŕ la réhabilitation, tandis que la complexité de la gestion consiste
en les complications qui se produisent ŕ cause des effets systémiques. Cet article
décrit le cas d'un jeune homme atteint de brűlures électriques partielles et ŕ toute
épaisseur en 65% de la surface corporelle dans les extrémités inférieures, le tronc,
et le crâne occipital et pariétal. Les Auteurs décrivent les phases successives de la
thérapie et les complications qui se sont manifestées, qui incluent une diarrhée
persistante et l'incapacité de tolérer les aliments solides. Tous les problčmes ne sont
pas encore résolus. Ce cas complexe de brűlures électriques dues ŕ la haute tension ne
sera pas pas facilement oublié par les Auteurs.
BIBLIOGRAPHY
Du G., Slater H,, Goldfarb I., Hammell
E: Influences of different resuscitation regimens on acute early weight gain in
extensively burned patients. Burns, 17.
This paper was
presented at the Third International
Conference on Burns and Fire Disasters, held in Palermo,
Italy in June 1995.
Address correspondence to: Ms Mary Jo
Cerepani
The Western Pennsylvania Hospital, Pittsburgh
Pennsylvania, USA. |
MBC becomes WHO
Collaborating Centre
Burn and fire management specialists
everywhere, and members of the MBC in particular, will learn with satisfaction and pride
thatthe World Health Organization has designated the Mediterranean Club for Burns and Fire
Disasters a WHO Collaborating Centre.
This is a clear recognition by the world's supreme health authority of the valuable
scientific, organizational and humanitarian contribution of the MBC to this painful and
difficult aspect of health management.
With the official title of WHO Collaborating Centre for Prevention and Treatment of
Burns and Fire Disasters, our association becomes the first and only scientific body
in the world to be so designated, a challenge that the MBC will meet with dignity,
determination and efficacy.
In its next issue the Annals will describe in greater detail the privileges and
obligations involved in such an important and prestigious accolade, in a field that now
well overflows the shores of the Mediterranean. |
|