| Annals of Burns and Fire Disasters - vol. X - n. 3 - September 1997
INTENSIVE DECOLONIZATION EFFECT ON THE MICROBIOLOGICAL FLORA
OF BURN PATIENTS ADMITTED TO A BURN INTENSIVE CARE UNIT
Herruzo-Cabrera R, Garcia-Torres V, Garcia-Caballero J,
Fernandez-Arjona M, Mariscal-Sistiaga F, Rey-Calero J.
Plastic Surgery, Intensive Care and Preventive Medicine
Services, La Paz University Hospital, Spain
SUMMARY. Selective intestinal
decolonization is one of the most controversial techniques for the reduction of infection
in burn intensive care units. In burn patients this technique can be used together with
nasal decolonization and intensive skin decolonization. Our objective was to cheek the
evolution in time of skin flora in critical burn patients and to establish whether the
burn infection was endogenous or not. Two hundred and eight burn patients from our
intensive burn unit were included in the study. The colonization of different areas
(pharynx, nose, G1, burn zone, and healthy skin) was studied every week. The colonization
vs burn infection predictive value was obtained. Staphylococcus aureus (SA) from
patients, doctors, and nurses was checked to discover any transmission route of this
micro-organism. It was found that in patients with intensive skin decolonization the
microbiological normal flora was better preserved. When the normal microbiological flora
disappeared, colonization by Pseudomonas aeruginosa (PA) occurred very frequently.
Colonization predictive value vs burn infection was low but in weeks 3 and 4 of
hospitalization it reached its maximum values (45% in PA). Burn colonization was
similar in different parts of the body. SA phagotyping showed that all patients
were colonized by a different micro-organism. It was concluded that intensive burn patient
decolonization was useful for the preservation of microbiological flora and to prevent
colonization and infection from other micro-organisms, mostly endogenously.
Introduction
In the first week post-burn, the wound is colonized by gram-positives'
from the hair follicles, but later gramnegative micro-organisms are predominant.
Gram-negatives come mainly from the gastrointestinal (GI) tract` and they are usually able
to infect distal body areas by going through the intestinal barrier by way of the
lymphatics and veins as far as the skin .
Staphylococcus aureus (SA) colonization comes from an exogenous source, such as
other patients' or the nose of the burn patient.
Neely et al." showed that Pseudomonas aeruginosa (PA) and Candida albicans
(CA) are present in the patient before colonization; in the temporal evolution of
colonization, PA is first, SA second, Staphylococcus epidermidis (SE) third,
and CA last.
Nonabsorbent intestinal antibiotics reduce intestinal micro-organisms and are useful in
the prophylaxis of GI surgery. They can also be used to reduce infection in burn patients
'although there is some disagreement on this point.'
The first intestinal decolonization',1 included oral aminoglycosides plus erythromycin
plus antifungal drugs; we prefer to replace erythromycin with polymyxin B.
Nowadays selective intestinal decolonization (SID) is used in the same way in neutropenic
patients" (polymixin B 800 mg + amphotericin B 1000 mg + tobramycin 300 mg p.o. per
day);" however Mason" used trimethroprim-sulphamethoxazole instead of
tobramycin. SID is used in traumatic patients and other intensive care patients.
There are various creams for skin prophylaxis in burn patients. The most popular are
silver sulphadiazine (1%), mafedine acetate (10%), and povidonc-iodine. In the light of
our experience 16 we prefer clorhexidine 0.5%.
This paper describes the temporal evolution of microbial colonization in burn patients and
considers whether or not the aetiology of the burn infection was endogenous.
Material and methods
For a period of three years we studied all patients admitted for two or
more days to the burn intensive care unit (BICU) at La Paz medical centre. Colonization
studies were developed twice per patient from different parts of the body (pharynx,
rectum, skin, body burn surface, etc.).
Our BICU is multidisciplinary, with 12 rooms (one per patient). We have written protocols
on manipulations that are published every two years.
Our main prophylactic techniques are wound debridement and surgical coverage, i.v.
antibiotic prophylaxis, microbiological patient flora monitorization, and intensive burn
decolonization (IBD).
IBD is divided into four parts: gastrointestinal decolonization: oral tobramycin 300
mg/day + nystatin 100,000-150,000 u/kg/day + polymyxin E 400 mg/day
- nasal decolonization: fusidic acid cream or chlorhexetidine 5%
- pharyngeal decolonization: hexetidine spray
- burn surface decolonization: chlorhexidine 0.5% cream (Rovi Lab.)
IBD should continue until total burn coverage. We do not use i.v.
prophylactic antibiotics other than surgical prophylaxis, except in electrical burns, when
we use penicillin 20 ml/day for two days.
Active epidemiological surveillance was practised with all patients.
We consider as skin infection cases in which the patient presents clinical features (fever
without any other sign of infection and negative blood cultures, defective scarring, etc.)
and microbiological features. We do not use burn surface biopsy as we prefer the
serniquantitative burn surface study," which gives basically the same results but is
a less aggressive procedure.
We represent the colonization-like prevalencel" in every week of the study as
follows: number of colonized patients x 100/number of patients admitted that week.
We perform microbiological monitorization in every patient once or twice a week. In these
procedures we look for possible pathogenous micro-organisms (PPM)" in the pharynx,
rectum, nose, and skin; we use agar blood, agar chocolate, and McConey with antibiotic
disk (cephalothin) and trimethoprime-sulphametoxazole);'I when these cultures do not
present PPM we diagnose as normal flora (NF).
We use the Crickett-Graph programme to calculate the colonization tendency lines and the
polynomial regression equation.
SA isolated from any patients and sanitary personnel were submitted to the National Center
of Microbiology in order to establish whether or not there was cross-transmission in our
unit.
We calculated positive and negative predictive values" (any infection vs burn surface
infection) when any PPM from the patient were isolated; these values enable us to know the
efficacy of the predictive values as risk factors for infection in our patients.
Results
Two hundred and eight patients were studied (mean age, 40.4 ± 1.3 yr;
mean body burn surface burned, 24.8 ± 1.5%; 46% on respiratory support; 100% on
antibiotics at some time).
Colonization
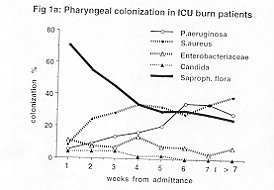
Pharynx (Fig. 1a). NF decreased by 50% in a week and a half
and by 70% in the fourth week. This reduction was due to SA colonization and subsequently
to PA. CA and Enterobacteriaceae have a very low colonization percentage.
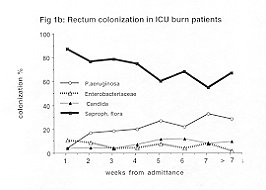
Rectum (Fig. lb). NF decreased 25% in the first month and
continued decreasing to 40% in the following months. PA is the most important colonizing
micro-organism.
 |
 |
| Fig. la - Pharyngeal colonization
in ICU burn patients. |
Fig. lb - Rectum colonization in
ICU burn patients |
|
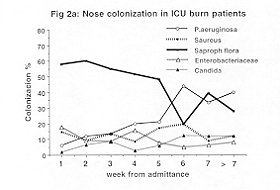
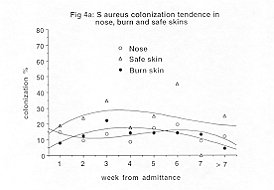
Nose (Fig. 2a). In the first week NF was reduced by 40% and
remained at 50% until the fifth week. NF was ducto PA and SA colonization. CA colonization
was about 10% after one month.
Healthy skin. Normal flora showed many changes in this area, but
usually decreased to around 40%. About 30% of the patients were colonized by SA.
Non-methicillin-resistant SA were the most important in the first week but subsequently
methicillin-resistant SA appeared.
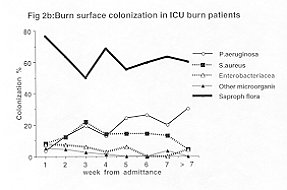
Body burn surface (Fig. 2b). NF decreased to 60% and remained
around this level. SA and PA were the most important micro-organisms. The SA were usually
methicillin-resistant.
 |
 |
| Fig. 2a - Nose colonization in ICU
burn patients |
Fig. 2b - Burn surface colonization
in ICU burn patients |
|
Table I shows colonization positive and negative predictive
values in different areas of the body. It is important to note that positive predictive
values were low and that the high levels occurred between the second and third weeks
(>45 % in PA and 25 % in SA). Mean positive predictive values were 17% in PA and SA and
11% in Enterobacteriaceae. Negative predictive values were very high (100% in many weeks).
| Time |
Micro-organism |
| P aeruginosa |
S. aureus |
Enterobacteriaceae |
| + Pv |
-PV |
+ PV |
- PV |
+ Pv |
- PV |
| Week 1 |
11.8% |
100% |
14.3% |
100% |
8,5% |
100% |
| Week 2 |
45.8% |
100% |
25% |
100% |
13% |
100% |
| Week 3 |
42.9% |
100% |
18.7% |
100% |
20% |
100% |
| Week 4 |
8% |
100% |
22.2% |
100% |
0% |
100% |
| Week 5 |
26.9% |
100% |
12% |
100% |
0% |
100% |
| Week 6 |
0% |
100% |
20% |
100% |
0% |
100% |
| Week 7 |
0% |
100% |
18.2% |
100% |
0% |
100% |
| Week 8 |
0% |
100% |
0% |
100% |
0% |
100% |
| Global |
17.8% |
100% |
17.4% |
100% |
11.8% |
100% |
|
Table 1 - Predictive values of P
aeruginosa, S. aureus and Enterobacteriaecae colonization versus burn infection by these
micro-organisms |
|
Colonization tendency
If we group all micro-organisms coming from any area of the body, we can see how these
bacteria colonized NE Fig. 3 shows a continuous decrease in NF from the first week
of admittance (50% in the first month and 40% in the second). PA increased every week from
the beginning up to 30% in the second month.
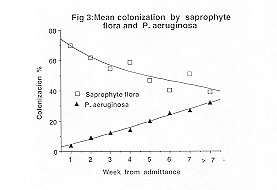 |
Fig. 3 - Mean colonization by
Saprophyte flora and P. aeruginosa. |
|
Pharyngeal, nose, and healthy skin vs body burn surface colonization
relationship
SA - Fig. 4a shows that SA colonization was similar in body burn surface,
healthy skin, and the nose, but was totally different in the pharynx.
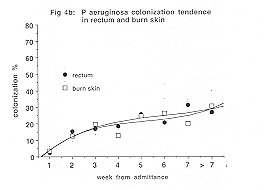
PA - Body burn surface and rectum colonization by PA were similar (Fig. 4b).
 |
 |
| Fig. 4a - S. aureus colonization
tendency in nose, burn, and safe skins. |
Fig. 4b - P. aeruginosa
colonization tendency in rectum and burn skins. |
|
Phagotyping
We compared SA isolated from different body areas in patients, nurses, and doctors. We
were unable to prove cross-transmission (patient-patient; patient-staff) except in one
case where we found the same SA in the nose of one nurse and the burn surface of one
patient. The nurse's nasal colonization was treated with clortexidine 0.5%.
Discussion
The temporal evolution of burn colonization and the aetiology of
certain micro-organisms like SA have not been well studied.
Sawhney et al.,11 in a five-year study, examined 342 patients with more than 20% BSA
burns. In the first two weeks SA colonization was the most important, while in the third
week PA was the predominant micro-organism. The burn was colonized by PA in 38% of cases,
Enterobacteriaceac in 14%, and SA in 37%.
We followed up our patients for eight weeks. In the first month we observed 15%
colonization by PA and SA, while in the second month SA increased and PA decreased.
Enterobacteriaceae and yeast were very unusual (5-8%) in the first month, after which they
disappeared.
Colonization by PA increased in other body areas up to 30%. If we compare the studies of
Deutsch' and Mason" with our own we can see that Deutsch found 93% burn colonization
by micro-organisms with an enteric source (PA 87%, Proteus 27%) and 57% SA. In the
Mason study 21% of burn colonization was by PA, 13% by Enterobacteriaceae (no Proteus),
9.5% by yeast, and 51% by SA. In our study, 18% of burn colonization was by PA, 12% by
SA, 4.5% by Enterobacteriaceae, and 2% by yeast; this proves that SID, as used by Mason
and ourselves, very effectively prevents colonization by gram-negative micro-organisms of
enteric origin.
We also believe that our SID could be even more effective than that of Mason to prevent
Enterobacteriaceae and yeast colonization. However, our results were better for SA because
we also developed nasal, skin, pharyngeal, and especially nasal colonizatioff with
chlorhexidine 0.5%, which is superior to silver sulphadiazine .15, 11 These
differences were not related to the gravity of the patient because although the mean BSA
was lower in our study, patient colonization with more than 30% BSA was similar.
In patients with 30% BSA, SID was more aggressive and as a result we found in these
patients 9% colonization by PA, 3% by Enterobacteriaceae, and 16% by SA.
Patient colonization had a very low predictive value for burn infection. In the second and
third week the relationship was 1: 2 for PA and less than I% for other
microorganisms. The negative predictive value was very high, i.e. there was no infection
without previous colonization.
Figs. 4a and 4b show that the micro-organisms usually came from the patient.
In our study, environmental bacteria were always different from the micro-organisms in our
unit.
SID also prevents respiratory and urinary infection, 15,24,25 and we therefore
think this should be a routine procedure.
 |
 |
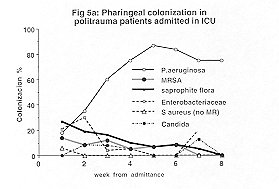
| Fig. 5a - Pharyngeal colonization
in polyLraumatic ICU patients. |
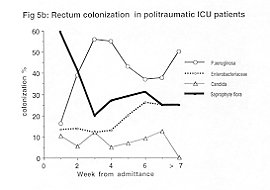
Fig. 5b - Rectum colonization in
polytraumatic ICU patients |
 |
 |
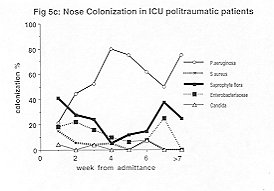
| Fig. 5c - Nose colonization in
polytraumatic ICU patients. |
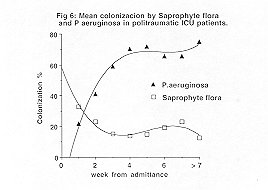
Fig. 6 - Mean colonization by
saprophyte flora and P. aeruginosa |
|
Figs. 5a and 5b show pharyngeal, nasal, and rectal
colonization. Comparing Figs. I and 2 we can see that there was an important
decrease in normal flora in the first two weeks and that usually PA was the main
colonizing micro-organism.
If we consider mean colonization in any body area, it can be seen, for instance, that in
polytraumatic patients (Fig. 6) there was an important decrease in normal flora in
the second week (70% colonization) followed by a slow increase (80% colonization)
in two months.
RESUME. La décolonisation intestinale sélective
constitue une des techniques plus controverses pour la réduction de l'infection dans les
unités des soins intensifs des brûlures. Dans les patients brûlés cette technique peut
être utilisée avec la décolonisation nasale et la décolonisation intensive de la peau.
Notre but était de contrôler l'évolution dans le temps de la flore de la peau chez les
patients brûlés en condition critique et d'établir si l'infection était endogène.
Deux cent huit patients brûlés provenant de notre unité de brûlures intensive ont
été étudiés. La colonisation de zones différentes (pharynx, nez, gastrointestin, peau
brûlée et saine) a été étudiée toutes les semaines. Nous avons obtenu la valeur
colonisation contre valeur prédictive de l'infection. Nous avons contrôlé le Staphylococcus
aureus (PA) chez les patients, les médecins et les infirmiers pour établir la route
possible de la transmission de ce micro-organisme. Nous avons trouvé que chez les
patients traités avec la décolonisation intensive de la peau la flore normale
microbiologique a été mieux conservée. Quand la flore microbiologique normale
disparaît la colonisation par Pseudomonas aeruginosa (PA) est très fréquente. La
valeur de la prédiction de la colonisation contre l'infection par la brûlure etait basse
mais pendant la troisième et la quatrième semaine de l'hospitalisation cette valeur a
gagné les valeurs maximales (45% pour PA). La colonisation de la brûlure etait
similaire dans les zones différentes du corps. La phagotypie de SA montrait que tous les
patients étaient colonisés par un micro-organisme différent. Les auteurs concluent que
la décolonisation intensive du patient brûlé est utile pour la préservation de la
flore microbiologique et pour prévenir la colonisation et l'infection par d'autres
micro-organismes, pour la plupart par voie endogène.
BIBLIOGRAPHY
- Deutsch D.H., Miller S.F., Finley R.H., Jr: The use of intestinal antibiotics to
delay or prevent infections in patients with burns. J. Burn Care Rehabil., 11: 436-42,
1990.
- Monafo W.W.: An overview of infection control. J. Trauma, 19: Suppl. 11: 879-80, 1979.
- Jarret F., Balish E., Moylan A., Ellerbe S.: Clinical experience with prophylactic
antibiotic bowel suppression in burn patients. Surgery, 83: 523-7, 1978.
- Van Saene H.F.K., Nicolai J.P.A.: The prevention of wound infections in burn patients,
Scand. J. Plast. Reconstr. Surg. Hand Surg.,13: 63-7, 1979.
- Tompkins R.G., Burke F.F.: Infections of burn wounds. In: Bennett J.E., Mandell G.L.,
Eds, "Hospital infections", 3rd ed., Boston Little Brown, 711-30, 1992.
- Deitch E.A., Berg R.: Bacterial translocation from the gut: a mechanism of infection. J.
Burn Care Rehabil., 8: 475-82, 1987.
- Hi M., Guang-Xia X., De Wong W., Ngao L.: Endogenous microbial dissemination following
severe burns in rats. Burns, 12: 325-9, 1986.
- Inoue S., Peck M.D., Alexander J.W.: Fungal translocation is associated with increased
mortality after thermal injury in guinea pigs. J. Burn Care Rehabil., 12: 19-22, 1991.
- Jones W.G. 11, Barber A.E., Minei J.P., Fahey T.J. 111, Shires III G.T., Shires G.T.:
Differential pathophysiology of bacterial translocation after thermal injury and sepsis.
Ann. Surg., 214: 24-30, 1991.
- Neely AX, Childress C.M., Maley M.P., Holder J.A.: Causes of colonization of autografted
burn wounds. J. Burn Care Rehabil., 12: 294-99, 1991.
- Manson W.L., Westerweld A.W., KlaseD H.J., Sanez E.W.: Selective intestinal
decontamination of the digestive tract for infection prophylaxis in severe burned
patients. Scand. J. Plast. Reconstr. Surg. Hand Surg., 21: 269-72, 1987.
- Manson W.L., Klasen H.J., Sauer E.W., Olieman A.: Selective intestinal decontamination
for prevention of wound colonization in severely burned patients: a retrospective
analysis. Burns, 18: 98102, 1992.Guiot H.F.L., van Furth R.: Partial antibiotic
decontamination. BML1:800,1977.
- Stoutenbeek C.P., van Saene H.K.F., Miranda D.R.: The effect of oropharyngeal
decontamination using topical nonabsorbable antibiotics on the incidence of nosocornial
respiratory tract infection in multiple trauma patients. J. Trauma, 27: 357, 1987.
- Selective decontamination of the digestive tract. Trialists' collaborative group.
Meta-analysis of randomised controlled trials of selective decontamination of the
digestive tract. BMJ, 307: 525-32, 1993.
- Herruzo-Cabrera R., Vizcaino-Alcaide M.J., Mayer R.F., Rey-Calero J.: A new in vitro
model to test the effectiveness of topical antimicrobial agents. Use of an artificial
eschar. Burns, IS: 35-8, 1992.
- Herruzo-Cabrera R., Garcia-Torres V., Rey-Calero J., VizcainoAlcaide M.J.: Evaluation of
the penetration strength, bactericidal efficacy and spectrum of the action of several
antimicrobial creams against isolated micro-organisms in a burn centre. Burns, 18: 39-44,
1992.
- "Guia para la prevenci6n y control e la infecci6n hospitalaria." Madrid,
Hospital La Paz, 1992.
- Herruzo-Cabrera R., Vizcaino-Alcaide M.J., Pinedo-Castillo C., Rey-Calero J.: Diagnosis
of the local infection of a burn through a semiquantitative recount of the eschar surface.
J. Burn Care Rehabil., 4: 639-41, 1992.
- Rothman K.J.: "Epidemiologia Moderna." Madrid, Ed. Diaz de Santos, 1987.
- Lennette E.H., Balows A., Hausler W.J., Truant J.P.: "Manual of Clinical
Microbiology" (3rd ed.). Washington, American Society for Microbiology, 1980.
- Rey-Calero J.: Metodo epidemiologico y salud de la comunidad. Madrid, Interamericana,
1989.
- Sawhney C.P., Sharma R.K., Kaushish R.: Long-term experience with 1% topical silver
sulphadiazine crearn in the management of burn wounds. Burns, 15: 403-6, 1989.
- Alvarado F., Herruzo R., Ruza F.: Descontaminaci6n intestinal como factor de protecci6n
en la preventci6n de infecci6n nosocomial en una UCI pediatrica. Sixth World Conf. on
Intensive and Critical Medicine, Spain, 1993.
- Herruzo-Cabrera R., Gonzales J.L., Garcia-Magan P., Rey-Calero J.: Nosocomial infection
in a neonatal intensive care unit and its prevention with selective intensive
decolonization. A multivariant evaluation of infective reduction. Eur. J. Epidemiol., 10:
573-80, 1994.
This paper was received on 15 May 1997.
Address correspondence to: Dr R. Herruzo-Cabrera
Departamento de Medicina Preventiva
Universidad Autonoma de Madrid
Cl Arzobispo Morcillo 4
28029 Madrid, Spain. |
MBC - PREVENTION
CAMPAIGN
The MBC, in the context of the activities laid down in its
statute and intended to promote burn prevention campaigns, has produced the following
videotapes:
- The Prevention of Burns in Children
- The Prevention of Electrical Burns in Everyday Life
- The Prevention of Electrical Burns at Work
- The Prevention of Industrial Disasters
- How to Defend ourselves from Fire
- How to Defend ourselves from Forest Fire
The tapes have been dubbed in English, French, Arabic, Italian,
Spanish, Greek and Turkish and come in two versions, U-MATIC and VHS. All the tapes are
available entirely free of charge to MBC Members who apply in writing to receive them
explaining their reasons and undertaking to use them exclusively to promote a burn
prevention campaign in their respective countries. Applications must be forwarded to the
MBC Secretariat. |
|