Annals of Burns and Fire Disasters - vol. X
- n. 3 - September 1997
USE OF DIESEL OIL IN
THE REMOVAL OF TAR FROM BITUMEN BURNS
AI-Hoqail R.
King Faisal University, King Fahd Hospital of the University, Al-Khobar, Saudi
Arabia
SUMMARY. Hot
tar burns mainly occur in workers in the paving and roofing industries. They present a
difficult clinical problem owing to the adherence of material to the underlying skin. In
the past, in Lebanon, diesel oil was widely used in the construction business in cases of
tar burns, with rapid removal and excellent results. Because of the unavailability of
solvents, diesel was applied in a recent case described in this paper. There was no
further damage to the underlying burn. A review of the literature revealed that diesel has
never been reported as a solvent for tar burns. Further research is recommended.
Introduction
Burns due to hot tar present a difficult
management problem because tar is difficult to remove without causing further injury to
the underlying burn.
Dickson et al. reported that in the Bradford Football Stadium fire, falling molten bitumen
was the cause of injury in some patients who substained mixed-depth scalp burns. Deep
dermal or full-thickness burns of the scalp were tangentially excised and skin grafted.'
In a nine-year review by James and Moss of 24 patients with such burns, sixteen required
operative treatment to achieve healing; no secondary reconstructive procedures were
performed. They suggested the following management principles:
- cool the bitumen continuously with cold
water until it hardens, in order to dissipate retained heat
- leave the bitumen intact except around the
eyes
- deroof tense blisters
The use of petrolatum -based ointments on the burn initially to dissolve
the tar into the dressings, over a period of 24-72 hours, is recommended as the most
effective and humane method of tar removal . There is no evidence in the literature
regarding the use of diesel oil to remove dried and adherent tar from bitumen burns. The
following case report, in which diesel oil was used for this purpose, is thus unique.
Case report
A 25-year-old Saudi
male substained tar burns in the face, left foreann, and hand while heating bitumen to
help in the roofing of his house. In the Emergency Room, the total body surface area
affected was found to be about 10%. The exact depth was initially difficult to assess, but
ome blistering was noted. The patient was given analgesia, and intravenous fluid therapy
was initiated. Solvents for tar were not available in the hospital at the time and
consequently the burn became dry and adherent.A chance conversation with an elderly
Lebanese family friend employed in the construction business suggested that diesel oil was
a fast and efficacious method for the removal of dried and adherent tar from bitumen burns
in construction workers. 1 asked the family to buy two litres of diesel oil, which they
brought about 24 hours later. Meanwhile, the patient remained without any kind of
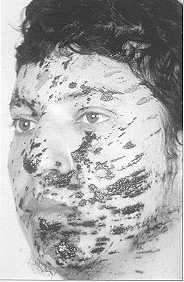
dressing. He was photographed just before and immediately after removal of the tar with
the diesel-soaked lap tapes (Figs. 1-6). The whole process took about 30 minutes. The
soaked lap tapes were applied and left on for a few seconds, after which the tar was
gradually wiped off the face and hand. The patient's only discomfort was a slight tingling
sensation at the end of the process. All the wounds were found to he second-degree. The
blisters were cleaned carefully without causing them to rupture. The patient's body was
washed with saline, and the burns were photographed and treated with fucidin toule and
fucidin-ointment-soaked gauze. The facial and foreann burns healed in four weeks and the
hand burns in five weeks. The patient was discharged after ten days and went on sick leave
for four weeks, after which he returned to normal work. Seven months later, complete blood
count and liver and kidney function tests continued to be within normal limits. Two years
later, the face was normal and without hyperpigmentation spots. There was a line of
hyperpigmentation on the left forearm. The fingers of the left hand showed scars in the
web spaces between the middle three fingers. Surgical intervention is planned.
 |
 |
| Fig.
I - Tar burn before diesel treatment. |
Fig.
2 - Immediately after tar removal
with diesel oil and body shower. |
|
Discussion
The major health problems in the
roofing trade are caused by the use of coal-tar pitch products. Severe eye and skin
irritations are frequent among roofers.' Contact burns due to thermoplastic road paint
also occur; this is used at similar temperatures to tar and bitumen, and spillage on to
skin causes similar contact burns. Most of these occupational burn injuries can be avoided
by observing the manufacturer's recommendations about the wearing of protective clothing.
Tar or asphalt, a residue of petroleum refining, is composed of paraffinic and aromatic
hydrocarbons and heterocyclic compounds containing sulphur, nitrogen and oxygen. It
becomes liquid when heated to 93 'C. However, it is often heated to over 232 'C when it is
used for roofing and paving. At these temperatures, molten tar causes deep burns.
Two-thirds of these burns involve 3 to 5% of the body surface, and only one-third involve
10% or more.
Ng D. et al.1 reviewed work-related burns between July 1989 and May 1990 (193 patients,
tar and asphalt burns representing 9.3%). Between July 1984 and 31 December 1991, 27
consecutive patients were admitted to the Grady Memorial Hospital Burn Unit requiring
treatment for hot tar burns. This group represented 1.4% of all admissions to this burn
unit. Ninety-six per cent were males. The mean age was 33.7 years. The mean burn extent
was 13.1% of total body surface area. Burn topography centred on the upper extremities and
hands. Forty-one per cent of the patients required a surgical procedure for their burn.
The mean hospitalization time for survivors was 16.6 days. The survival rate was 92.6%.
Both the patients who died had large burns and/or pre-existing medical problems. Hot tar
burns occur in predictable circumstances and appear to be preventable. They account for
only a small fraction of all admissions.' In this case report the patient was a young male
who sustained a 10% surface burn involving the face, left forearm, and hand.
 |
 |
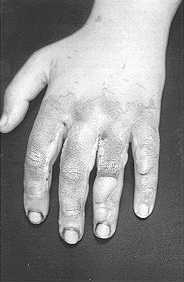
| Fig.
3 - Before treatment |
Fig.
4 - After removal of tar. |
|
A review of the literature
shows that various substances have been used in the management of tar burns, including
mayonnaise," butter," and the surface acting agent polyoxyethylene sorbitan
(Tween 80, Sigma, St Louis, Mo) or polysorbate (Sigma), either by itself or in combination
with an antibiotic ointment (neomycin sulphate). These have been found to be safe and
effective means of tar removal.
Liquid solvents such as kerosene, gasoline, acetone and alcohol have been found to be
generally ineffective in removing tar and can damage local tissues, occasionally producing
systemic toxic effects due to absorption. Neosporin (polymyxin B sulphate/neomycin
sulphate/gramicidin) cream has been found to dissolve tar, thereby facilitating removal,
Its emulsifying agent, polyxyethylene sorbitan has excellent Iyophilic and hydrophilic
properties and is thus a very effective non-ionic surface active agent. The polysorbate
lowers surface tension and promotes micelle formation at the cell surface, thus clearing
the bond between the cell surface and the adherent material. Because of the polysorbate's
hydrophilic action, the emulsified tar can be washed off with water. Neosporin ointment
(polymyxin B sulphate-zinc bacitracin-neomycin sulphate) with a petrolatum base also
dissolves tar but is less effective than the cream, which has a polysorbate base.
Polyoxyethylene 20 sorbitan mono~olcate (Tween 80, the 80 referring to the average
molecular weight of the polyethylene glycol polymer) is another readily available
polysorbate that serves as an emulsifying agent and a dispersant in cosmetics and coal tar
ointment used for treating skin disorders.
An anecdotal report from an old family friend who works in the construction business
suggested that diesel oil was used safely and efficiently by workers in that industry.
There is no evidence in the literature regarding the use of diesel oil in the removal of
adherent dried tar after bitumen burns. 1 used diesel oil in my patient, and it proved
highly effective and safe.
 |
 |
| Fig.
5 - Before treatment. |
Fig.
6 - After removal of tar. |
|
Tar burns involving more
than 10% of the body surface area are likely to be the most serious, requiring intravenous
fluid resuscitation and a petrolatum-based ointment applied to the burn in the initial
stages.
The following recommendations represent a summary of the comments received from numerous
physicians involved in burn care, both in the United States and elsewhere, in response to
an inquiry from the United Union of Roofers, Waterproofers and Allied Workers, as directed
by their International President Roy E. Johnson, regarding the initial treatment of hot
bitumen burns.
Immediate on-site
care
Cool the bitumen with water (preferably cold) to limit tissue damage
and prevent further spread of the bitumen
Cooling should continue only until the bitumen has hardened and
cooled. Body hypothermia must be avoided
Adherent bitumen should not be removed "in the field" but
only at a medical facility by qualified personnel
Definitive care by
medical personnel
Bitumen adherent to skin blisters after cooling should be removed
with the blister epithelium in th e course of initial cleansing and debridernent
Bitumen adhering to unblistered tissue should in general be left in
place and covered with a liberal application of a petrolatum or animal-fat-based material
(petrolatum per se, lanolin, mineral oil, and antibacterial ointments were used by
various respondents to the questionnaire). Antibiotic-containing ointments, which may
limit bacterial proliferation on the burn, were most widely used by respondents
The adherent bitumen should then be dressed and the dressing removed
on a daily or more frequent basis. Repeated ointment and dressing applications
Observation of these guidelines will
enable the providers of first aid and initial care for patients with bitumen bums to
reduce tissue injury, decrease pain, prevent infection, and minimize the complications and
disability resulting from these job-related injuries.
Tar bums have evolved tremendously in their management and it seems that diesel oil is a
gentle and rapid relieving agent after which local management is routine. Further research
on the utility of this substance in tar bums is needed.
RESUME. Les brűlures
causées par le bitume chaud touchent principalement les ouvriers employés dans
l'industrie du pavage et de la toiture de la maison. Ces brűlures présentent un
problčme ŕ cause de l'adhérence du matériau ŕ la peau sous-jacente. Dans le passé,
au Liban, on faisait grand usage du gazole dans l'industrie de la construction pour
traiter les brűlures causées par le bitume, avec une élimination rapide et des
résultats excellents. A cause de la non disponibilité de solvants, dans un cas récent
décrit dans cet article, on a utilisé le gazole. La brűlure sous-jacente n'a pas subi
d'autres dommages. Un contrôle de la littérature scientifique a indiqué que le gazole
n'a jamais ętre décrit comme solvant dans les brűlures causées par le bitume. Il
faudrait effectuer des recherches plus approfondies.
BIBLIOGRAPHY
- Demling R. H., Buerstatte W.R., Perea A.: Management of hot
tar bums. J. Trauma, 20: 242, 1980.
- Dickson W.A., Sharpe D.T., Roberts A.H.: Burns, 14: 151-5,
1988.
- James N.K., Moss A.L.: Review of burns caused by bitumen
and the problems of its removal. Burns, 16: 214-6, 1990.
- Schiller W.R.: Tar burns in the southwest. Surg. Gynecol.
Obstet., 157: 38-9,1983.
- Emmett E.A.: Cutaneous and ocular hazards of roofers.
Occup.Med., 1: 307-22, 1986.
- Riely P., Regan P.J., Budny P.G., Roberts A.H.: Contact
bums due to thermoplastic road paint. Burns, 17: 400-1, 1991.
- Bose B., Tredget T.: Treatment of hot tar bums. CMA
Journal, 127: 21-2, 1982.
- Ng D., Anastakis D., Douglas L.G., Peters W.J.:
Work-related burns: 6-year retrospective study. Burns, 17: 151-4, 199 1.
- Renz B.M., Sherman R.: Hot tar bums: twenty-seven
hospitalized cases. J. Burn Care Rehabil., 15: 341-5, 1994.
- Shea P.C., Jr., Fannon P.: Mayonnaise and hot tar burns. J.
Med. Assoc. Ga., 70: 650-60, 1981.
- Tiernan E., Harris A.: Butter in the initial treatment of
hot tar bums. Burns, 19: 437-8, 1993.
- Pruitt B.A., Jr., Eldich R.F.: Treatment of bitumen burns.
Arm. Emerg. Med., ll: 697,1982.
Acknowledgements.. 1 wish to express my
sincerest thanks and appreciation to Mr Abdulla Driskell and Mr Atif, the two librarians
at King Fahd Hospital of the University, for their special enthusiasm, interest and
continuous support extended to me during my research by providing reference materials. My
thanks also go to Professor Yaw Adu-Gyarnfi for his assistance during the editing stage.
| This paper was received on 15 May
1997. Address correspondence to: Dr
Rola Al-Hoqail
PO. Box 116, Al-Khobar
31952 Saudi Arabia
Tel.: 3.8642840; Fax: 3.8647262 |
|