| Annals of Burns and Fire Disasters - vol. X
- n. 3 - September 1997
ANATOMICAL STUDY OF
THE MEDIAL SEPTOFASCIAL FLAP OF THE LEG - ITS POSSIBLE CLINICAL APPLICATIONS
Al-Sayed Mandour
Ismail
Plastic and
Reconstructive Unit, Faculty of Medicine, Tanta University, Tanta, Egypt
SUMMARY. Most
anatomical and injection studies on the septocutaneous vessels of the leg have been
performed without separation of the septocutaneous flap as an island-pedicled flap. Using
observations on work done in our Unit with the distally based adipofascial flap in the leg
and foot, we studied the anatomy of the medial septofascial flaps by an injection study on
cadaver after separation of the flaps from the surrounding skin. Seventeen limbs were
examined in the study. Our results showed that the subfascial plexus is more important
than the suprafascial plexus if the flap is used as an island-based flap on the lower
septal vessel. If the adipofascial flap is used as an island flap, the fatty layer does
not prove a good surface to carry the split-skin graft until after the formation of
granulation tissue from the perforating vessels. However, if this fatty layer is removed
(septofascial flap), it can be a good surface to carry a split-skin graft, owing to the
good blood supply of the fascia. The distally based septofascial flap without the skin and
subcutaneous fat can reach any distance, from the midleg to the great toe, and can be a
vehicle to carry a split-skin graft, thus solving many clinical problems in the lower leg
and foot, such as chronic ulcers and deep burns. This is the basis of research currently
in progress in our unit.
Introduction
With regard to skin circulation, some strong anatomical data support
the assumption that septocutaneous vessels are at least as important as musculocutaneous
and axial vessels. Several types of fasciocutaneous flaps can be based on septal
pedicles.1-1 Most anatomical studies on the septocutaneous vessels of the leg describe the
fascial network as being composed of two layers, subfascial and suprafascial, and consider
the suprafascial layer to be more important than the subfascial plexus.'-' Bearing in mind
research already conducted in our Unit using the distally based adipofascial flap in the
leg and foot,' we studied the anatomy of the medial septofascial flaps by an injection
study of cadavers after separation of the flaps from the surrounding skin.
Material and methods
Seventeen limbs were dissected for the arterial supply of the medial
septocutaneous flaps of the leg. Ten limbs were from formalin-preserved cadavers, six were
from fresh cadavers, and one was amputated following an accident. Injection studies were
performed on the seven fresh limbs. The diameters of the septocutaneous arteries were
measured, as well as their distance from the medial malleolus.
Technique
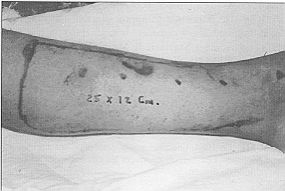
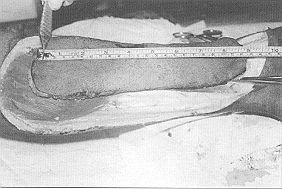
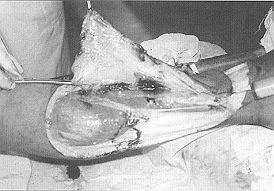
The flap was marked on the skin and raised with the deep fascia (Figs. 1,2). The septal
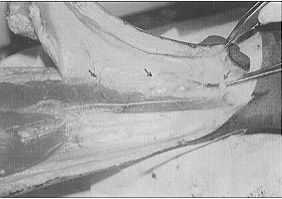
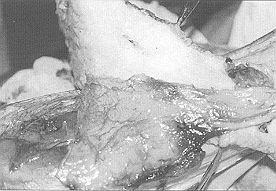
branches were dissected, and their origin, course and distribution identified and left
intact (Figs. 3,4). The lowermost septal branch was cannulated at its origin and
injected with 20 ml methylene blue or India ink (Fig. 5). Seven limbs were injected
through the lowermost septocutaneous vessel (three after separation of all septal branches
except the lowest and four before ligation and separation of the other vessels).
 |
 |
| Fig. I
- Marking the flap (25 x 12 cm). |
Fig. 2 -
Dissection of flap together with deep fascial layer (starting from posterior part) |
|
 |
 |
| Fig. 3
- Dissection of medial septocutaneous vessels in fresh cadaver. |
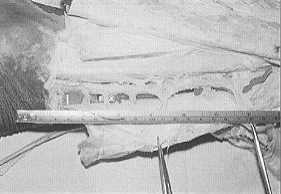
Fig. 4a
- Formalin-preserved leg. Six septocutaneous vessels arising directly from posterior
tibial vessels.
Lowermost vessel 6 cm and uppermost vessel 18 cm from medial malleolus. |
 |
Fig. 4b -
Formalin-preserved leg.Six septocutaneous vessels arising directly from
posterior tibial vessels.
Lowermost vessel 6 em and uppermost vessel 18 em from medial malleolus |
|
Results
Anatomical findings
The septal vessels are direct branches of the posterior tibial artery (Figs. 3,4a/b);
they do not originate from collateral vessels. Each septocutaneous artery has one and
sometimes two venae comitantes (Fig. 4b). These veins directly join the deep trunk. We
found three septocutaneous vessels in five limbs, four vessels in four limbs, five vessels
in four limbs, and six vessels in four limbs (Figs. 3,4). The distance of their origin
measured from the tip of the malleolus was 4 cm for the lowermost one and 18 cm for the
uppermost one. The uppermost of these vessels pierces the fascia, pressing through the
tibial origin of the soleus just behind the medial border of the tibia. The lowermost
medial septocutaneous vessel becomes superficial after passing between the flexor
digitorum longus and soleus muscles and the Achilles tendon (Fig. 4).
The external diameters of the arteries varied from 0.5 to 1.7 mm. Arteries of larger
diameters were found in the middle of the leg (Fig. 4b).
Results of injection study
Limbs injected before separation and dissection of the skin and
subcutaneous fat showed good perfusion of the dye to the skin, dermal and subfascial
plexuses. Dissection of the skin and subcutaneous fat from the fascia showed faint
colouration of the suprafascial plexus, and fine vessels could be seen in the fat layer (Figs.
5,6).
Limbs injected after cutting and ligation of the middle and upper septal vessels also
showed good perfusion of the skin, dermal and subfascial plexuses. However, when the skin
and subcutaneous fat were dissected from the fascia, the suprafascial plexus could not be
visualized, the fine vessels in the fat layer became fewer, and three or four perforating
branches could be seen traversing the fat layer without forming any branches (Figs.
7,8).
In all cases, the subfascial plexus was more prominent and well vascularized (Fig. 9).
 |
 |
Fig. 5 -
Lowermost septal vessel cannulated
and 20 ml dye (methylene blue) injected. |
Fig. 6 -
Good perfusion of dye to skin and dermal plexus and faint cotouration of superfascial
plexus. |
 |
 |
| Fig. 7 -
The suprafascial plexus cannot be visualized. Two perforating branches can be seen
traversing fat layer without forming any branches to the fat layer. |
Fig. 8
- Good visualization of subfascial plexus in all cases. |
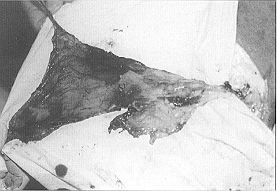 |
Fig. 9 - Good
visualization of subfascial plexus in all cases. |
|
Discussion
The coverage of distal soft tissue and bony defects of the leg has long
been recognized as a difficult clinical problem. Distally based fasciocutaneous flaps with
majorarteries in their pedicles have been described. However, these flaps have the
disadvantage of necessitating the sacrifice of a major limb artery. Also, the reversal of
venous flow in this type of flap increases the degree of venous compromise
The use of local fasciocutaneous, septocutaneous, myocutaneous and free flaps is often
associated with significant donor site defects and is cosmetically unacceptable for the
majority of the patients. Gumener et al. designed a distally based pedicled
fasciocutaneous flap from the calf to cover soft tissue defects in the malleolar region
and heel. Medial island septocutaneous flaps for the repair of soft tissue defects have
been used in our Unit for the last eight years.` The island adipofascial flap based on
septocutaneous perforators for resurfacing distal lower limb defects was the basis of a
study that we conducted. However, we noticed partial graft loss whether the graft was
placed on the fatty layer or on the reverse surface. For this reason we decided to perform
an anatomical study of the medial island fasciocutaneous flap based on the lower
septocutaneous vessels.
Our results showed good perfusion of the whole flap. Removal of the skin will however
affect the blood supply of the fatty layer (Fig. 7). The results also showed that
the subfascial plexus is larger and more prominent than the suprafascial plexus, contrary
to the findings of Carriquiry et al. This may be explained by the fact that in
Carriquiry's work the injection studies were performed without separation of the flap,
which might affect the haemodynamics inside the flap. Our results also explain why
Jayaraman," Mathivanan and Ramakrishnam," and Arianayagam," when describing
fascial, inferiorly based turnover flaps, attributed their vascularization to the abundant
vascular supply in the under surface of the deep fascia. Lees and Townsend" were the
first to report the use of the pedicled fascial flap based on septocutaneous perforators
of the posterior tibial artery for repair of a distal lower limb defect (two cases). If
this flap is raised as an island on the lower septal vessel, it will have a wide arc of
rotation (figs. 10/a/b/c/d).
 |
 |
Fig. 10a -
Wide arc of rotation of medial
septofascial flap from midleg to great toe. |
Fig. 10b - Wide are of
rotation of medial septofascial
flap from midleg to grat toe. |
 |
 |
Fig. 10c - Wide arc of
rotation of medial
septofascial flap from midleg to great toe. |
Fig. 10d - Wide arc of
rotation of medial septofascial
flap from midleg to great toe. |
|
On the basis of the above findings we can make the following
conclusions:
the medial island septofascial flap has a good blood supply, mainly
from the subtascial plexus and partly from the suprafascial plexus, and it can be a good
surface to carry split-skin graft for the solution of many problems in the lower leg and
foot
island septocutaneous flaps should be used without separation of the
skin from the flap
turnover of the island adipofascial flap and the positioning of the
split-skin graft on the under surface of the fascia affect the subfascial plexus, owing to
the thickness of the fatty layer, and the use of fascial flap alone is preferred
Island septofascial flaps have the following advantages:
simplicity of raising the flap
significant reduction in donor site morbidity
either side of the fascia can be grafted
the flap is useful on the dorsurn of the foot as it provides a
surface under which tendons can freely glide
RESUME. La plupart des �tudes anatomiques et d'injection
sur les vaisseaux septocutan�s de la jambe ont �t� effectu�es sans la s�paration du
lambeau septocutan� comme lambeau � p�dicule en �lot. En utilisant des observations
sur des recherches faites dans notre Unit� avec le lambeau adipofascial � base distale
pour la jambe et le pied, nous avons �tudi� l'anatomie des lambeaux septofasciaux
m�dians � travers une �tude d'injection sur le cadavre apr�s la s�paration des
lambeaux de la peau environnante. Dix-sept membres ont �t� examin�s dans l'�tude. Nos
r�sultats ont montr� que le plexus subfascial est plus important que le plexus
suprafascial si le lambeau est employ� comme lambeau � base en �lot sur le vaisseau
septal inf�rieur. Si le lambeau adipofascial est employ� comme lambeau en �lot, la
couche grasse ne se r�v�le une bonne surface pour porter la greffe d'�paisseur variable
qu'apr�s la formation du tissu granuleux depuis les vaisseaux perforants. Cependant, si
cette couche grasse est �nlev�e (lambeau septofascial), cela peut se r�v�ler une bonne
surface pour porter la greffe d'�paisseur variable, � cause du bon afflux de sang dans
la fascia. Le lambeau septofascial � base distale sans la peau ni la graisse
sous-cutan�e peut s'�tendre � toutes les distances, du milieu de la jambe au gros
orteil. Il peut en outre constituer un v�hicule pour porter la greffe d'�paisseur
variable pour r�soudre beaucoup de probl�mes cliniques de la jambe inf�rieure et du
pied, comme par exemple les ulc�res chroniques et les br�lures profondes. C'est la base
des recherches que nous conduisons actuellement dans notre Unit�.
BIBLIOGRAPHY
- Rocha A.M.., Zhenman S.T., Zhiguang S.P.: Experimental study and clinical use of the
fasciocutaneous flap. Plast. Reconstr. Surg., 78: 19,1986.
- Ponten B.: The fasciocutaneous flap. Its use in soft tissue defects of the lower leg.
Br. J. Plast. Surg., 34: 215, 1981.
- Donski P.K., Fogdestam I.: Distally based fasciocutaneous flap from the sural region. A
preliminary report. Scand. J. Plast. Reconstr. Surg., 17: 191, 1983.
- Thatte R.I., Laud N.: The use of the fascia of the lower leg as a rollover flap. Its
possible clinical applications in reconstructive surgery. Br. J. Plast. Surg., 37: 88,
1984.
- Carriquiry C., Costa M.A., Vasconex L.O.: An anatomic study of the septocutaneous
vessels of the leg. Plast. Reconstr. Surg., 76: 354, 1983.
- Cormack G.G., Lamberty B.G.H.: A classification of fasciocutaneous flaps according to
the patterns of vascularization. Br. J. Plast. Surg., 37: 80,1984.
- Pearl R.M., Johnson D.: The vascular supply to the skin. An anatomical and physiological
reappraisal. Part 11. Ann. Plast. Surg., 11: 196, 1983.
- Haertsch P.A.: The blood supply to the skin of the leg. A post-mortern investigation.
Br. J. Plast. Surg., 34: 470, 1981.
- Atef A. Allam: The distally based adipofascial flap in the leg and foot. M.Sc. thesis
for the Master's Degree in Surgery, Faculty of Medicine,Tanta University, 1995.
- Barclay T.L., Gordosa E_ Sharpe D.T., Rochett D.J.: Repair of the lower leg injuries
with fasciocutaneous flaps. Br. J. Plast. Surg., 35: 127, 1982.
- Tolhurst D.F., Haeseker B., Zeeman R.J.: The development of the fasciocutaneous flap and
its clinical applications. Plast. Reconstr. Surg., 71:597, 1983.
- Gumener R., Zbrodowski A., Montadon D.: The reversed fascial flap in the leg. Plast.
Reconstr. Surg., 88: 1034, 1991.
- Shalaby H.A., Mandour S., Higazi M., El-Khalifa M.A., Ayad H.:15 .Distally based
medial island septocutaneous flap for repair of soft tissue defects of the lower leg. Br.
J. Plast. Surg., 44: 178, 199 1.
- Jayaraman V: Fascial turn-over flaps in full thickness chronic burn ulcers. Transactions
of Int. Cong. Plast. Surg., pp. 126-8, New Delhi, India, March 1987.
- Mathivanan T., Mathangi Ramakrishnant K.: Fascial turnover flaps in full-thickness
defects. Transactions of Fourth Asian Cong. Plast. Surg., p. 41, Kuala Lumpur,
Malaysia, March 1988.
- Arianayagam C.: Inferiorly based reverse fascial and fasciocutaneous flaps. Transactions
of Fourth Asian Cong. Plast. Surg., p. 42, Kuala Lumpur, Malaysia, March 1988.
- Lees V., Townsend P.L.G.: Use of the pedicled fascial flap based on septocutaneous
perforators of the posterior tibial artery for repair of distal lower limb defects. Br. J.
Plast. Surg., 45: 141.
This paper was presented at the Ninth
Meeting
of the MBC held in Tunis in May 1996.Address
correspondence to: Dr Al-Sayed Mandour Ismail
Plastic and Reconstructive Unit, Faculty of Medicine
Tanta University
Tanta, Egypt. |
1998 AWARD
THE TANNER-VANDEPUT-BOSWICK BURN PRIZE
The Tanner-Vandeput Burn Prize (now the
Tanner-Vandeput-Boswick Burn Prize) was started in 1984 by Dr J.C. Tanner of Atlanta,
Georgia, co-iriventor with Dr. Jacques Vandeput of the Tanner-Vandeput mesh dermatome. The
Prize was conceived and established to promote the aims of the International Society for
Burn Injuries and to motivate individual investigators to perform research, undertake
patient care and treatment, and attempt to solve other aspects of the burn problem. In
1984 the ISBI Executive Committee voted to accept Dr Tanner's offer to work with the ISBI
in coordinating the Prize, which consists of a cash payment and a gold and diamond pin.
The Prize is awarded at each Quadrennial Congress of the ISBI. The International Burn
Foundation was created to promote and administer the Prize. In 1991 Dr Tanner requested
that the name be changed to the "Tanner-Vandeput-Boswick Burn Prize" to reflect
the contributions ofDr John Boswick, who has been Chairman of the Foundation Board
ofDirectors since inception. The first award was presented to Dr Ian Alan Holder of
Cincinnati at the 7th ISBI Congress in Melbourne in 1986. The second award was presented
to Dr Fortunato Benaim of Buenos Aires at the Sth ISBI Congress in New Delhi in 1990. The
third award was presented to Dr John E Burke of Boston at the 9th ISBI Congress in Paris
in 1994. The next award will be presented at the 10th ISBI Congress to be held in November
in Israel. The Prize consists of a gold pin and a cash payment anticipated to be in excess
of $ 100,000. The Prize will go to a person (or persons) who in the opinion of the Prize
Committee has made an outstanding contribution to any aspect of the burn field. This could
be a specific achievement or might represent a body of work over a period of years. The
recipient does not have to be a physician or a member of the ISBI. Nominations for the
1998 Prize may be made by colleagues of those who have made such major contributions, or a
candidate may make application on his own behalf. Anyone interested in making a nomination
should request an application form from the International Burn Foundation at the address
below.
INFORMATION REQUIRED TO APPLY FOR THE 1998 PRIZE:
1. Completed application
2. Letter of nomination
3. Description of work
4. Current CV
5. Letters of support from colleagues
DEADLINE FOR SUBMISSION OF APPLICATIONS: JANUARY
30,1998
CONTACT: Dr John Boswick
Chainnan, Board of Directors International Burn Foundation
P.O. Box 24386
Denver, CO 80224 USA
Phone: (303) 839-1694 Fax: (303) 839-1695 |
|