| Annals of Burns and Fire Disasters - vol. X - n. 4 - December 1997
BURNS IN THE ELDERLY. EPIDEMIOLOGY
AND MORTALITY: ANALYSIS OF 53 CASES
Bortolani A., Barisoni D.
First Division of Plastic and Reconstructive Surgery
and Burn Units, Istituti Ospitalieri di Verona, Verona, Italy
SUMMARY. Over
a four-year period (May 1991-May 1995) 53 patients aged over 60 years and with total
burned surface area >20% or full-thickness burn >10% were admitted to the Verona
Burn Centre, Italy. Flame burns were most commonest cause of injury, and hot liquids,
especially bath-water, and gas explosions were also aetiologically significant. Using
hypertonic solutions, we achieved satisfactory urine output and the reduction of
post-resuscitation complications. In order to reduce patient morbidity and mortality in
patients with preexisting cardiopulmonary diseases we used continuous positive airway
pressure and early respiratory physiotherapy. Systemic antibiotic prophylaxis was used in
many cases. In our experience early excision and grafting, in haemodynamically stable
patients, reduces mortality. Our policy for the elderly burned patient is based on use of
hypertorric sodium solution, early excision and grafting, nutritional support, and the
prevention of pulmonary complications. Mortality remains high, but is lower than in other
reports.
Introduction
Elderly patients continue
to present a high mortality rate. Restricted physiological reserves, together with
pre-existing diseases of the heart, lungs and kidney, may significantly impair the
patient's ability to respond appropriately to stress in the event of major burn injury.
This study was carried out in order to evaluate the possibility of enhancing survival in
elderly burned patients.
Patients and
methods
A review was made of 386
admissions to the Verona Burns Centre over the period May 1991-May 1995. Of these, 53
patients (27 males and 26 females, equal to 14% total admissions) were aged age over 60
years. The mean total burned surface area (TBSA) was > 20%, or full-thickness burn
(FTB) was > 10%. Forty-five patients had pre-existing diseases. Cardiovascular and
respiratory diseases were the most frequent and caused the greatest number of
complications, with the highest mortality. Continuous positive airway pressure (CPAP) of
2.5-5 cm H20 was applied for twenty minutes every two hours in a group of patients to
prevent respiratory complications. Physiotherapy and in many cases systemic antibiotic
prophylaxis following ABG were also used.
One group (30 patients) was resuscitated using the Baxter formula and 23 patients were
infused with a hypertonic saline solution (Na requirements */215 for the first 24 h). The
groups had a similar Roi index.
(*Na requirements = 0.6 x body weight x TBSA)
Results
Epidemiology
Most of the accidents took place in the home (45 cases); six occurred in a nursing home,
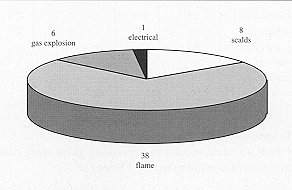
one at work, and one in a car crash. Flame burns were commonest cause of injury (55%). The
improper use of flammable agents and hot liquids, especially bath water, together with gas
explosions, were also aetiologically significant. One patient was admitted for electrical
burns (Fig. 1). Forty-five patients (85%) had a pre-existing disease and this was the
cause of burns in six patients; of these two "collapsed" owing to a
cardiovascular accident, three had neurological problems, and one was unconscious as a
result of a hyperglycaernic coma when the burn was sustained.
|
Fig.
1 - Aetiology of burns in 53 elderly patients |
|
Table I shows the
severity of the burns in relation to age. Out of 29 patients with severe burns (TBSA >
25% or FTB >15%), eleven died (40%), while only six deaths occurred in the 24 patients
with moderate burns (TBSA 20-25 % or FTB 10- 15 %).
| |
Moderate
Pts/Dtbs |
Severe
Pts/Dths |
81-90
Tot/Dths |
| 60-70 |
12/2 |
14/3 |
26/5 |
| 71 -80 |
8/3 |
11/7 |
19/10 |
| > 80 |
4/1 |
4/1 |
8/2 |
| Total |
24/6 |
29/11 |
53/17 |
|
Table
I - Age, size of burns, and mortality in 53 elderly patients |
|
Fluid resuscitation
All fifty-three patients received early fluid replacement during the first 48 hours
post-burn. Of the thirty patients who received colloids and electrolyte solutions,
twenty-five had a pre-existing disease and fourteen presented complications during
admission. Of the twentythree patients who received hypertonic saline resuscitation,
twenty had pre-existing diseases and only five had complications (Table II). There
was a significant difference between the two groups as regards the complication rate (p
< 0.05). No statistically significant changes were observed in the mortality rate.
Mortality was very much influenced by the presence or absence of pre-existing diseases,
whatever the type of resuscitation.
| |
Baxter
formula
(Roi0.51) |
% |
Hypertonic
saline solution
(Roi 0.77) |
% |
| With diseases |
|
|
|
|
| N. patients |
25 |
|
20 |
|
| Complications |
14 |
56% |
5 |
25% |
| Deaths |
11 |
44% |
6 |
30% |
| Without diseases |
|
|
|
|
| N. patients |
5 |
|
3 |
|
| Complications |
I |
|
I |
|
| Deaths |
0 |
|
0 |
|
|
| Table II -
Comparison between two different type of resuscitation in 53 elderly patients.
Complications and mortality |
|
Respiratory
complications
CPAP was determinant in preventing pulmonary complications and reducing mortality (Table
III).
| |
N.
pts |
Complications |
% |
Deaths |
% |
CPAP
(Roi 0.53) |
22 |
6 |
27% |
4 |
18% |
Without CPAP
(Roi 0.40) |
31 |
13 |
42% |
14 |
45% |
|
Table
III - Complications and deaths in 53 elderly patients treated with or without CPAP |
|
Surgical treatment
Surgery within ten days was performed in 22 patients (mean Roi index 0.34). In this
group four patients died (18%), while late surgical treatment in 21 patients (mean Roi
index 0.45 ) was associated with a mortality rate of 28% (6 deaths). The difference in
mortality between the two groups was significant (p < 0.05) but it did not take into
account the Roi prognostic index (Table IV). The duration of hospital stay in the
two groups was similar
| |
pts |
Average
Age |
Average
%TBSA |
Mortality
% |
Stay
(Days) |
Early
excision
(Roi 0.34) |
22 |
75 |
25 |
4 18% |
32 |
Late
excision
(Roi 0.45) |
21 |
71 |
30 |
6 28% |
45 |
|
Table
IV - Influence of surgical timing on mortality and hospital stay in 53 elderly
patients |
|
Discussion
The increased
average lifespan of human beings has resulted in a gradual increase in the number of aged
persons. Geriatric patients with accompanying chronic or debilitating diseases present
special problems, as many of them live alone and perform their housework efficiently until
their dexterity and responsiveness deteriorate with age. General conditions like low
stress response, impaired immunological function, and pre-existing cardiopulmonary
diseases are responsible for the increase in mortality in elderly patients. Also, atrophy
of the skin' and dermal appendages, as well as poor microcirculation, influences the depth
of the lesion and slows down healing processes.
Pulmonary complications related to nosocomial infection and to bed confinement are very
dangerous for these patients.' Prevention of such complications is therefore mandatory,
and in our burns centre CPAP and breathing exercises, associated when necessary with
antibiotic therapy, are routine forms of treatment. In this manner, in our patients we
reduce both mortality (18% vs 45%) and complications (27% vs 42%). Fluid resuscitation in
aged patients requires appropriate monitoring" of hourly urinary output, CVP, and
other haemodynamic parameters. Hypertonic saline solutions reduce the amount of fluid
infused and the complication rate, and maintain a good hourly urine oUtpUt.14 Various
researchers have suggested that excision on or before day 5 has a benefical effect on
total hospitalization time and mortality." In our series patients with severe burn
injury were treated with early excision and grafting before day 10, leading to a reduction
in mortality from 28% (late excision) to 18% in patients operated before day 10 post-burn.
No difference was observed between the two groups as regards length of hospital stay. One
question remains open: is there a relationship between mortality and delayed admission to
a burns centre? Our experience did not provide an answer, since early admission regarded
more severe patients with a higher mortality rate, while late admission (after 24 h)
concerned precautions: less extensive burns with a better prognosis. 19,20 The present
report makes the following points:
- mortality is more closely correlated to size, depth of
burn, and pre-existing disease than to age (Tables I,II)
- resuscitation with hypertonic sodium solution can reduce
complications but not mortality (Table II)
- combined treatment with CPAP and antibiotic prophylaxis
reduces the complication rate and mortality; this is particularly true in patients with
pulmonary diseases (Table III)
- early excision and grafting reduce mortality but not the
length of stay (Table IV)
- the mechanisms and the severity of injury are related to
sensory impairment (smell, sight, hearing), living alone, the wearing by women of
loose-fitting garments while cooking, and dozing while smoking.
To reduce these
risks we recommend the following greater attention to control of the environment the use
of smoke and gas detectors in the home garment flammability regulations stricter
regulations on smoking in institutions such as nursing homes, general hospitals and
psychiatric centres, and the introduction of self-extinguishing cigarettes
RESUME. Pendant
une période de cinq ans (mai 1991 - mai 1995) les Auteurs ont étudié 53 patients âgés
de plus de 60 ans atteints de brûlures dans plus de 20% de la surface corporelle ou 10%
à toute épaisseur hospitalisés dans le Centre de Brûlés de Vérone (Italie). La cause
la plus commune des brûlures était les flammes; aussi les liquides chauds
(particulièrement pour le bain) et les explosions étaient importants du point de vue de
l'étiologie. Utilisant des solutions hypertoniques ils ont obtenu une production d'urine
suffisante et la réduction des complications de la phase post-réanimatoire. Pour
réduire la morbidité et la mortalité des patients qui présentaient des maladies
cardiopulmonaires préexistantes, les Auteurs ont employé la pression positive continue
des voie aériennes et la physiothérapie précoce. La prophylaxie antibiotique
systémique a été employée en divers cas. Selon l'expérience des Auteurs Fexcision
précoce et les greffes réduisent la mortalité dans les patients hémodynamiquent
stables. Pour les patients âgés, ils recommandent l'emploi de solutions de sodium
hypertoniques, l'excision et la greffe précoce, le support nutritionnel et la prévention
des complications pulmonaires. La mortalité reste étévée mais elle est plus basse par
rapport à d'autres résultats.
BIBLIOGRAPHY
Tajerina C., Baena P., Mirabet V.:
Massive burns: a study of epidemiology and mortality. Burns, 20: 51, 1994.
Lewandowski R., Pegg S., Fortier K.,
Skimmings A.: Burn injuries in the elderly. Burns, 19: 513, 1993.
Slater H.: Burn injury in the aged
patient. Burns, 7: 74, 199 1.
Herd B.M., Herd AX, Tanner S.B.:
Burns to the elderly: a reapprai sal. Br. J. Plast. Surg., 40: 279, 1987.
Housinger T., Saffie J., Ward S.:
The elderly patient with burns. Conservative approach to the elderly patient with burns.
Am. J. Sing., 149: 817, 1984.
Bing-Guo L., Wei-shia H., Tsi-siang
H.: Causes of death in aged burn patients: analysis of 36 cases. Burns, 16: 207, 1990.
Petro J., Belger D., Salzberg C.A.:
Burn accidents and the elderly.What is happening and how to prevent it. Geriatrics, 44:
26, 1989.
Glasheen W.P., Attinger E.O., Anne
A.: Identification of the high risk population for serious burn injuries. Burns, 9: 193,
1983.
Griffiths RX: Burn injury in the
aged patients. Burns, 7: 365, 1981.
Pruitt B.A., Mason A.D., Hunt J.L.:
Burn injury in the aged or high risk patients. In: "The aged and high risk surgical
patients", Siegel J.H., Chodoff P., Grime & Stratton, New York, 198 1.
Herndon D.N., Barrow R.E., Linares
H.A.: Inhalation injury in burned patients. Effects and treatment. Burns, 12: 357, 1986.
Hadjiiski 0.: Brulures chez les
personnes ag6es. Ann. Medit. Burns Club, 7: 63, 1994.
Agarwal N., Salisbury R.:
Physiological profile monitoring in burned patients. J. Trauma, 23: 577, 1993.
Bowser-Wallace B.H.: Hypertonic
lactated saline resuscitation of severely burned patients over 60 years J. Trauma, 25: 22,
1985.
Burke LE, Boindoe C., Quiriby WC.:
Primary burn excision and immediate grafting. Amethod shortening illness. J. Trauma, 14:
389,1974.
Deitch E.A., Clothier RX: Burns in
the elderly. An early surgical approach. J. Trauma, 23: 891, 1983.
Scott-Conner C.E., Love R, Wheeler
W: Does rapid wound closure improve survival in older patients with burns? Am. Surg., 56:
26, 1990.
D'Arpa N., Napoli B., Masellis M.:
The influences of a variety of parameters on the outcome of the burn disease in elderly
patients. Arm. Medit. Burns Club, 6: 15, 1993.
Baux S., Mimoum M., Saade H.: Burns
in the elderly. Burns, 15: 239, 1989.
Zoeh G., Meissl G., Bayer S., Kyral
E.: Reduction of the mortality rate in the aged burn patient. Burns, 18: 153, 1992.
This
paper was received on 16 June 1997.
Address correspondence to:
Alberto Bortolani M.D.
Prima Divisione di Chirurgia Plastica e Centro Ustioni
Istituti Ospitalieri di Verona, Italy. |
|