| Annals of Burns and Fire Disasters - vol. X - n. 4 - December 1997
SEVERE
COMPLICATIONS IN BURN TRAUMA - A CASE REPORT
Hrubá J., Kónigová R.
Third Medical Faculty of Charles University,
Prague, Czech Republic
SUMMARY. A 52-year-old patient suffered burns
in 69% T13SA. The cause of the accident was a flare-up of his clothing, which was soaked
in diluent fluid. Prior to the trauma the patient had been suffering from a duodenal
ulcer. Prophylaxis of stress bleeding was performed by H2 blockers. In spite of
this treatment, there was massive bleeding from the stomach, and by day 16 post-burn
surgical treatment became indispensable. The bleeding continued and the patient had to be
treated with terlipresin and subsequently with somatostatin. The side-effect of this
treatment was a hypertensive reaction and the onset of severe, haemodynamically
significant arrhythmia. The patient was treated with intravenous nitroglycerin and a
variety of antiarrhythmics for 46 days. The burned areas were treated by necrectomies and
transplants. A further complication was osteomyelitis of the right hip bone. The cause of
the thromboeytosis remains unclear. Rehabilitation of the patient still continues.
Introduction
Burn trauma is always a cause of tremendous stress for the
afflicted person. Proof of this is the eleven-fold elevation of the catecholamine level.
Bleeding from the gastrointestinal tract and other multiple stress complications can
develop several hours or days following the trauma, caused by shock hypoxia, inhalation
trauma, endotoxinaemia, and even iatrogenic factors. The psychological causes of stress
include intense pain, the need to cope with an unexpected life situation, apprehension of
repeated surgery, and fear of further life stigmatized by burn sequelae.
Case report
A 52-year-old man suffered burns in 69% T13SA on 24 October 1994.
The cause of the accident was the flare-up of his clothing soaked in diluent fluid. Prior
to the trauma the patient had been suffering from ulcer disease. First aid was performed
in a local hospital where the patient was also treated with dexamethasone (total dose 12
mg). The patient was transported to the Burn Centre in Prague the same day, 8 h after the
accident. Releasing incisions were performed and the burn areas were covered with
dressing; an intravenous line, nasogastric tube, and urine catheter had already been
inserted. The patient was treated in the usual way: fluid resuscitation, including
crystalloids, and subsequently plasma, analgesics, intravenous heparin (10,000 u/day) for
the prophylaxis of thromboembolic disease, together with H2 receptor inhibitors
(cimetidine 1200 mg/day) and enteral feeding to prevent stress bleeding.
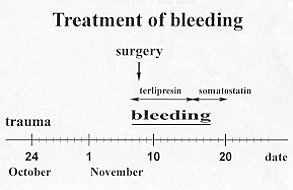
In spite of all these preventive measures, massive bleeding from the stomach with
haematemesis and melaena occurred on November 7. Treatment with terlipresin was commenced
(3 mg/24 h). Because of the failure of conservative therapy, surgical treatment was found
the next day to be indispensable. A bleeding ulcer penetrating to the hepatoduodenal
ligament was found in the lesser ventricular curvature. Suturing was performed. Bleeding
continued and the patient had to be treated with with terlipresin for the following seven
days. In view of the continued bleeding, terlipresin was replaced by somatostatin (6 mg/24
h) for 3 days, 4 mg/24 h for 1 day, and 1 mg/24 h for 1 day). During the haemorrhage
period the patient was given 28 blood transfusions. The therapy with somatostatin was
successful in the treatment of the gastric bleeding, but severe cardiac complications
occurred during the terlipresin treatment (Fig. 1).
|
Fig. I - Treatment of bleeding. |
|
Hypertensive reactions and severe, haemodynamically significant
tachyarrhythmias appeared. Hypertension was treated with nifedipine and nitroglycerin
intravenously for 46 days. As the supraventricular tachyarrhythmias produced hypotension
and consequently circulatory failure, various antiarrhythmic drugs were repeatedly applied
in high doses (digoxin, verapamil, ajmaline, amiodaron and pindolol). There were temporary
but significant diffuse ischaernic changes in the patient's ECG (horizontal depressions of
ST segment and negativization of T waves). Localized myocardial lesions were not found.
The conjunction of terlipresin application and of the rise of hypertension with
haernodynamically significant arrhythmias was obvious.
The burned areas were treated by avulsion, necrectomy, xenotransplantation and, finally,
autotransplantation.
During the course of hospitalization the patient was treated with several antimicrobial
drugs because of infections in the burn wound and the respiratory and urinary tract; the
iliofemoral joint and bone were also affected (Fig. 2). Different types of microbe
were cultivated (Staphylococcus epidermidis, Staphylococcus aureus, Klebsiella
pneumoniae, Pseudomonas aeruginosa, Enterococcus faecium, Enterobacter cloacae,
Acinetobacter calcoaceticus, Serratia liquefaciens, Xantomonas maltophilia, Proteus
mirabilis, Escherichia coli, and Aspergillus).
| TIENAM |
3.11
- 15.11 |
| DIFLUCAN |
12.12
- 28.12 |
| PRIMOTREN |
24.11
- 1.12 |
| CIPRINOL |
2.12
- 7.12 |
| FORTUM |
7.12
- 12.12 |
| TIENAM |
13.12
- 23.12 |
| TARGOCID |
13.12
- 27.12 |
| AMIKACIN |
23.12
- 16.1 |
| COLISTIN |
27.12
- 7.2 |
| TARGOCID |
31.1
- 7.2 |
| AZACTAM |
31.1
- 8.2 |
| DALACIN |
27.4
- 19.6 |
|
Fig. 2 - Antimicrobial drugs. |
|
Six months after injury the patient started physiotherapy out of bed. A
gastroscopic investigation was performed and scarring was found in the healed ulcer. An
echocardiographic investigation was carried out on the same day. The kinetics of all the
myocardial walls was quite normal and no impairment of myocardial function was found.
Fourteen days later the patient started to complain of pain in the right hip. Coxitis was
diagnosed and Staphylococcus attreus was cultivated from the joint. Antimicrobial
treatment was recommenced and correct external fixation was carried out because of
dislocation of the right lower extremity towards the pelvis.
Another unusual phenomenon was a change in the thrombocyte count. The decreased number of
thrombocytes was due to burn shock and massive bleeding. But the increase in the number of
thrombocytes to more than one million is hard to explain. The patient was treated with
dipyridamole and low-molecular heparin for this abnormality (Fig. 3).
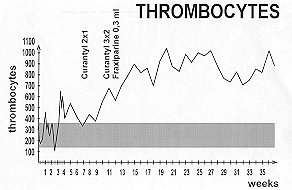 |
Fig. 3 - Thrombocytes. |
|
Discussion
Four questions arise with regard to this patient:
- Was the gastric bleeding preventable?
- Were the haernodynamically significant arrythmias the consequence of previous medical
therapy?
- What was the aetiology of the right hip bone inflammation ?
- What was the cause of the thrombocytosis?
For the prophylaxis of gastrointestinal tract ulceration one can use as
soon as possible food administration, antacids, H2 receptor inhibitors, and sucralphate .4
This patient was treated from the time of admission to the Burn Centre with H2 receptor
inhibitors - cimetidine intravenously in continual doses and enteral feeding through a
nasogastric tube. Gastric bleeding in this patient, who was suffering from ulcer disease,
occurred in spite of all the preventive measures. At present we use mostly ranitidin and
sucralphate in patients with a history of ulcer disease.
The prevalence of ischaernic heart disease among males in their fifties is high. It can be
manifested by heart failure or arrhythmias. Severe vasoconstrictive hypertension and
haemodynamically significant supraventricular tachyarrhythmias appeared in our patient
during and after terlipresin therapy. Terlipresin is a synthetic polypeptide - an analogue
of natural hormone from the posterior lobe of the hypophysis. It has extreme
vasoconstrictive effects. Somatostatin is a 14-amino acid oligopeptide that inhibits
gastrointestinal endocrine and exocrine secretion and motility as well as resorption
within the digestive tract.
The ECG ischaemic changes in this patient were only temporary, since the echocardiographic
investigation carried out in a later period showed a normal picture. For this reason the
cardiac complications were considered a probable consequence of the previous medical
therapy.
The right hip joint inflammation could have been caused by haematogenic transport of
microbes or per continuitatem with the joint. It is difficult to establish what
type of microbial translocation was more probable in this patient because of the multiple
surgical procedures performed in the right lower limb.
The explanation of the remarkable thrombocytosis is unclear. The aggregability of
thrombocytes was normal and the finding in bone marrow was also normal. The patient will
be followed up in the haematology department for the possibility of the development of
myeloproliferative disease without any relation to the burn trauma.
RESUME. Un patient âgé de 52 ans a été atteint de
brûlures en 69% de la surface corporelle. La cause de l'accident était la flambée de
ses vêtements imbibés de diluant. Précédemment le patient souffrait d'ulcères
duodénales. Les Auteurs ont effectué la prophylaxie de l'hémorragie par stress
moyennant les bloquants de l'H2, mais malgré ce traitement une hémorragie massive
gastrique s'est produite et 16 jours après la brûlure le traitement chirurgical s'est
révélé indispensable. Lhémorragie a continué et il fallait traiter le patient avec le
terlipresin et ensuite par la somatostatine. Ueffet collatéral de ce traitement a été
une réaction hypertensive et des arythmies hémodynamiquernent significatives. Le patient
a été traité pendant 46 jours avec la nitroglycérine intraveineuse et divers
médicaments antiarythmiques. Les zones brûlées ont été traitées avec des
nécrectomies et des transplantations. Une autre complication successive a été
l'ostéomyélite du col du fémur droit. La cause de la thrombocytose n'est past claire.
La réhabilitation du patient continue.
BIBLIOGRAPHY
- Haberal M., Ozdemir A., Bayraktar B. et A: Gastrointestinal and renal complications in
burn patients. Ann. Medit. Burns Club, 6: 26, 1993.
- Yuesheng H., Ao L., Zongcheng Y: A prospective clinical study on the pathogenesis of
multiple organ failure in severely burned patients. Burns, 18: 30, 1992.
- Klein D., Moshkovitz Y, Lipin 1. et a].: Arterial embolization in the treatment of
Curling's ulcer bleeding in a burn patient. Burns, 19: 447, 1993.
- LaggnerA.N., Lenz K., GraningerW. et al.: Stress bleeding prophylaxis - sucralfate vs
ranitidine. Abstracts 5th International Sucralfate Symposium, Miami, USA, 1993.
- Lefer A.H.: Interaction between myocardial depressant factor and vasoactive mediators
with ischernia and shock. Am. J. Physiol., 252: 193, 1987.
- Arevalo V.A., Del Campo B.T., Gomez B.G. et el.: Hypercoagulation in burn
patients - efficacy of thromboembolic prophylaxis.
- Pandit S.K., Malla C., Zarger H.U. et a].: A study of bone and joint changes secondary
to burns. Burns, 19: 227, 1993.
This paper was presented at the
Third International Conference on Burns and Fire Disasters
held in Palermo, Italy in June 1995.
Address correspondence to: Prof. J. Hrubd and Prof. R. KOnigova
Third Medical Faculty of Charles University
Prague, Czech Republic. |
MBC - PREVENTION CAMPAIGN
The MBC, in the context of the activities laid down in its statute and intended to
promote burn prevention campaigns, has produced the following videotapes:
- The Prevention of Burns in Children
- The Prevention of Electrical Burns in Everyday Life
- The Prevention of Electrical Burns at Work
- The Prevention of Industrial Disasters
- How to Defend ourselves from Fire
- How to Defend ourselves from Forest Fire
The tapes have been dubbed in English, French, Arabic, Italian, Spanish, Greek and
Turkish and come in two versions, U-MATIC and VHS. All the tapes are available entirely
free of charge to MBC Members who apply in writing to receive them explaining their
reasons and undertaking to use them exclusively to promote a burn prevention campaign in
their respective countries. Applications must be forwarded to the MBC Secretariat. |
|