| Annals of Burns and Fire Disasters - vol. X - n. 4 - December 1997
RADIOLOGICAL DIAGNOSTICS OF PULMONARY COMPLICATIONS IN BURN REANIMATION:
POSSIBILITIES AND PROBLEMS
Dmitrienko O.D.(1), Golimbievskaya TA.(2),
Trofimova T.N., Kossovoy A.L.
St Petersburg Medical Academy of Postgraduate
Studies, St Petersburg, Russia
(I) Department of Radiology;
(2) Department of Thermal Lesions
SUMMARY.
This paper considers minimal burns with a potentially favourable prognosis, the effects of
which were much aggravated by the presence of inhalation trauma. In the group of patients
considered, 17 fatalities were expected, against an actual number of 27. Radiological
investigations provided a considerable amount of interesting information, as the pulmonary
complications could be predicted by evaluation of the dynamics of the radiological
changes. This facilitated early intensive therapy.
Introduction
Our research shows that even in cases of
minimal burn area the presence of inhalation trauma played a highly negative role in the
final outcome (71% lethal). In the cases described in this paper, a lethal outcome was
expected on the basis of the prognosis in 17 cases, while in reality 27 deaths were
recorded. Radiological investigation of the patients' early stage proved to be highly
informative. Pathological pulmonary changes appeared as early as 24 h post-injury. The
earliest indications of the development of a pathological process in the lung were an
increase and a deformation in the pulmonary pattern in roof segments (central
localization) as a result of vascular hyperaemia, caused by hypertransfusion. This is
typical in haemodynamic pulmonary oedema. The localization of changes in pulmonary pattern
in the periphery of the pulmonary fields was typical of respira~ tory distress syndromes,
as a result of haemodynamic violation of the pulmonary capillaries.
The most characteristic form of lesion in fires and burn accidents is a skin burn of
various type combined with inhalation trauma (IT). Thermochemical affections of the
respiratory system and poisoning due to combustion products remain the primary causes of
early death among fire victims. Early diagnosis of damage to the respiratory tract is
difficult - it is not possible to determine the degree of damage and thus establish a
proper prognosis. Current investigative methods of IT diagnostics, e.g. bronchoscopy,
pulmonary scanning using isotope 133x,, and blood gas analysis, are not usually
implemented in burn centres in country areas owing to the lack of necessary equipment.
Also, implementation of these methods in the event of the mass admission of burn victims
would be extremely complicated. The role of radiological methods of the diagnostics of
pulmonary complications in fire victims is thus very important.
As long ago as 1947, Schatrkir noted a wide variety of radiological changes in the victims
of a fire disaster in a Boston night club. The role and the optimal timing of the
radiological analysis of IT-affected lungs remain controversial.Dynamic radiological
analysis of pulmonary complications in the pre-clinical period provides a possible line of
conduct for early intensive therapy in the presence of such complications .3,4 Most
problems arise in diagnos~ tics and in the differential diagnostics of pulmonary corn~
plications such as the respiratory distress syndrome (RDS) in adults. The object of this
paper is to study the radiological pattern of critical diffusive lesions of the vascular
lung channel in fire victims and the development of criteria for differential diagnostics
of RDS and haemodynamic pulmonary oedema (HPO).
Materials and methods
A complex clinical, laboratory,
radiological and forensic medical analysis was made of 31 fire victims with both average
and high-degree inhalation damage (Table I).
Inhalation trauma was diagnosed in all 31 victims on the basis of anamnesis, facial
burns, and changes in the mucous membrane of the nose, mouth and pharynx, and also on the
basis of clinical symptoms (unconsciousness, cough with saturated phlegm secretion,
cyanosis) and laboratory tests (carboxyhaemoglobin and blood gas level).
More than 10% of the patients suffering from deep burns received anti-shock therapy
(colloids) and protein transfusion (3 to 8 litres) in the first three days. Medical
therapy (heart preparations, analgesics, heparin, Lasix, corticosteroids and vitamins) was
also performed.
Patient
groups |
Number
of patients |
Average
age
(yr) |
Area deep
lesions
(%) |
Thermochemical
lesion of
respiratory organs |
CO2
poisoning |
Death
prognosis |
Middle
time of life treatment |
Death |
Life |
1 |
7 |
50.6 |
10 |
7 |
5 |
5 |
22.1 |
34.4 |
2 |
17 |
52.1 |
10-45 |
17 |
14 |
15 |
13.5 |
2.5 |
3 |
7 |
34.7 |
45 |
7 |
5 |
7 |
6.5 |
|
All |
31 |
|
|
31 |
24 |
27 |
21 |
18.4 |
|
Table I
- Fire victims with various lesions as regards degree of damage and prognosis |
|
Medication was introduced through
catheters in the upper and lower cava veins (five patients also received rnedication
through the aorta). Hyperbaric oxygenation (through a microtracheostoma) and artificial
lung ventilation (usually 1-2 days before death) were administered during treatment.
The radiological symptoms of severe diffuse lesions of the pulmonary vascular channel were
compared with data obtained from the study of 113 patients with other primary pathologies
leading to pulmonary complications, such as:
combined trauma (32 cases)
abdominal pathology (7 cases)
blood loss (5 cases)
heart attack (10 cases), etc.
Experimental data were obtained through
the study of 33 dogs. The experiments were conducted under conditions of hexenal i.v.
anaesthesia (20-30 mg/kg mass) and artificial ventilation of the lungs. The model for
toxic pulmonary oedema was developed by i.v. injection of silver nitrate at a dose of 1.2
mg/kg-1. Mixed pulmonary oedema was simulated by pressing the dogs' kidney vessels, the
flow through which was re-established after three hours' exposure. Haemodynamic oedema was
created by raising arterial and venous perfusion pressure in lungs ventilated and perfused
through the pulmonary artery. Sodium chloride was added to reduce colloid osmotic
pressure. The pulmonary conditions were monitored by radiological, histological and
ultrastructural methods, and also on the basis of the gas content and acid-base balance of
the blood, haemodynamic data, and gravimetric results.
All the patients underwent chest radiography on days 1, 3, 5 and 7 days post-injury.
Results
Our research shows that even in cases
of minimal burn area (potentially favourable prognosis) the presence of IT played a highly
negative role in the final outcome (71% lethal). On the basis of the prognosis, a lethal
outcome was to be expected in 17 cases, while in reality there were 27 fatalities.
RDS was detected radiologically in 18.7% of the burned patients with IT. In 50% of the
cases different stages of cardiac pulmonary oedema (interstitial, alveolar) were found. In
21.8% of the cases severe pneumonia was observed. A combination of RDS and HPO was
detected in 74.2% of the cases, of RDS and severe pneumonia in 12.9%, and of HPO and
severe pneumonia in 12.9% (Table II).
Groups of
patients |
Number
of
patients |
Number
of
Roentgeno-
grams |
Anisotropic
|
Isotropic
|
Roentgeno-
metrics |
RDS |
62 |
138 |
17 |
34 |
17 |
Haemody-
namic pulm.
oedema |
49 |
81 |
9 |
18 |
9 |
Severe
pneumonia |
33 |
132 |
5 |
7 |
2 |
Total |
144 |
351 |
41 |
77 |
36 |
|
Table II
- Analysis of findings |
|
In severe pneumonia, focus infiltration of
high intensity with fuzzy contours was detected with reactive changes of the roots, and
increased pulmonary vascular pattern. There was no correlation between the development of
pneumonia and area of deep skin lesions - 25% of patients affected had developed pneumonia
by day I post-trauma, 44% by day 3, and 30% by day 5. Changes due to pneumonia were
detected radiologically not earlier than days 23 post-burn. A bilateral process in the
basal segments was detected more often.
With the development of RDS, a strengthening of the pulmonary vascular pattern with fuzzy
contours and network deformation due to the vascular component was detected (Table
III). In 54% of the cases enlargement and fuzziness of the bronchial walls were
detected.
| Symptoms |
% |
| Focal infiltration changes in periphery of
pulmonary fields and in gravitation-dependent zone |
85.7 |
| Poor structural pulmonary roots |
77.3 |
| Decreased pulmonary pneumatization |
69.5 |
| Bullous emphysema |
63.3 |
| Diffusion of increasing fuzzy vascular
pulmonary pattern with network deformation |
61.2 |
| Enlarged, fuzzy bronchial walls |
54.4 |
| Air bronchography |
32.0 |
|
Table III -
Frequency of radiological symptoms in patient with respiratory distress syndrome |
|
Nonsignificant malfunctioning in the
haemodynamics of the pre-capillary part of the pulmonary network of the blood circulation
was noted. This was expressed by enlargement of the diameter of the artery of the third
segment (up to 5.5 mm) and by widening of the descending branch of the right pulmonary
artery (up to 18 mm). All subsequent stages of the pathological process in the lungs were
characterized by the appearance of focal infiltrative shadows. A typical observation in
the majority of cases was the localization of the changes on the periphery of the
pulmonary fields as well as in the gravitation-dependent segments (60%) (Figs. 1-3). The
appearance of focal and infiltrative shadows was followed by the breach of the pulmonary
root structure in 93% of the observations and by the appearance of subpleural oedema along
the horizontal interlobular border (36%). There was an increase in the changes in the
bronchial walls.
The diminishing of the process was characterized by a decrease in the quantity and
intensity of focal and infiltrative changes in 13 patients. These patients had dominant
discrete shadows that started to disappear on days 20-24.
 |
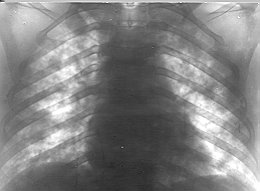 |
| Fig. 1 -
Alveolar pulmonary oedema. |
Fig. 2 - Respiratory
distress syndrome. |
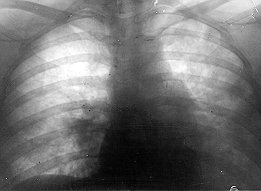 |
Fig. 3 -
Acute pneumonia and alveolar pulmonary oedema |
|
The multiplicity of the causes of RDS
gives the radiological changes specific characteristics. Thus, in patients with acute
surgical abdominal pathology, the radiological signs - even in the early stages of RDS -
are noncharacteristic disc collapses, pleural effusion, and high diaphragm position. This
indicates a catastrophe in the abdominal cavity and makes it difficult to evaluate the
changes. In cases of mixed trauma the radiological interpretation become more difficult
owing to various traumatic radiological characteristics, such as emphysema, fractures,
pneumothorax, hydrothorax, etc. Differential diagnostics of the pulmonary injury and RDS
is not so difficult because of the local nature of the traumatic changes. In patients with
pulmonary complications due to blood loss and massive haemotransfusions, radiological
findings show evidence of increasing volume blood circulation and the development of right
ventricle deficiency (significant increase in size of right atrium). These features are
not common in cases of RDS. A similar picture was detected in burn patients.
The radiological pulmonary picture in burned patients with haemodynamic pulmonary oedema
was different from that seen in RDS patients. Results of a comparative analysis of the
radiological picture in cases of RDS and of HPO are summarized in Table IV.
| |
|
RDS(%) |
HPO(%) |
| Lung roots |
No change |
27.8 |
- |
| |
Decreased structure of pattern |
64.5 |
87.5* |
| |
No differentiation |
7.6 |
12.5 |
Vascular
pulmonary
pattern |
No change |
13.3 |
- |
| |
Strengthened and deformed |
77.1 |
1 1_5 _* |
| |
Uneven strengthening |
- |
50.0 |
| |
No differentiation |
6.5 |
18.7 |
| Bronchial walls |
Enlarged, fuzzy |
24.5 |
13.0* |
Interlobular
pleura |
Enlargement |
9.7 |
49.7* |
| * = P
< 0.5 |
|
Table IV -
Radiological characteristics of RDS and HPO |
|
Changes in the lung roots were the
earliest signs of interstitial pulmonary oedema of haemodynamic origin. In cases of RDS
these were unchanged in almost 28% of the cases. An analysis of the pulmonary picture
showed that venous hypertension was typical of interstitial pulmonary oedema, but not of
RDS. Kerley lines were detected only in cases of interstitial pulmonary oedema.
Progressive haemodynamic damage led to alveolar pulmonary oedema. The most pronounced
changes were detected in near-roof pulmonary segments. The pulmonary roots were markedly
changed and undifferentiated in 12.5% of the cases. Total or infiltrative change with
large shadows was characteristic of haemodynamic pulmonary oedema. Liquid evacuation from
mobile parts of the lung caused the appearance of a band-like pneumatized parenchyma above
the diaphragm. This symptom was observed mostly in patients with haemodynamic pulmonary
oedema (30%). The picture of air bronchography was not typical in these conditions. In
haemodynamic pulmonary oedema there was a faster dynamic in cases of progressive change as
also in cases of resolution of the process after adequate intensive therapy.
The data obtained from animal models and clinical observations support the difference in
radiological expression of haemodynamic pulmonary oedema and RDS.
C-ray investigations in experimental toxic oedema showed that vasodilatation and an
increased number of focal shadows in cases of hyperhydration and hypoxaemia were the
earliest signs of pulmonary vessel permeability lesions.
Optical image post-processing made it possible to perform a detailed analysis of the
radiological picture (Table V). RDS was characterized by diffuse strengthening and
deformation of the pulmonary picture and vascular pattern focal shadows, which were
localized in the periphery of the pulmonary fields. The presence of large unstructured
zones correlated with the focus of the oedema, with central localization, was typical of
haemodynamic pulmonary oedema. A similar but relatively localized picture was observed in
cases of pneumonia. In general, implementation of optical image post-processing made it
possible to increase precision of diagnostics to 90.4%, specificity to 87.5%, and
sensitivity to 92.4%.
| Symptoms |
RDS
(%) |
HPO
(%) |
Pneumonia |
Diffusive strengthening
of vascular pulmonary pattern |
64.7 |
20 |
- |
| Changes in interstitial tissue |
88.2 |
80 |
80 |
Oederna near bronchial
interstitial space |
47.0 |
80 |
- |
| Disc collapses |
76.5 |
- |
- |
Focal shadows, alveolar oedema
and effusion of blood |
58.8 |
20 |
60 |
| Emphysema of the acinus |
70.5 |
60 |
60 |
| Foci of the infiltration |
- |
100 |
100 |
| Pleural effusion |
- |
20 |
40 |
|
Table V -
Frequency of radiological symptoms in optical image postprocessing of acute respiratory
insufficiency |
|
The results of the research are summarized
in the proposed differential diagnostic algorithm. Effective differential diagnostics is
only possible if based on the stages of process of the development in the lungs. Thus, two
large groups can be highlighted on the basis of the presence or absence of focal and
infiltrative changes in the lungs. Diagnostics is based on the detection of haemodynamic
malfunctioning or on increasing permeability of the pulmonary capillaries. These become
the major differential diagnostic criteria in cases of absence of focal infiltrative
pulmonary changes. Kerley lines of the pulmonary roots and heart signs are additional
criteria.
Conclusions
- Radiological investigation of patients in the early stages
post-injury proved to be highly informative.
Pathological pulmonary changes appeared as early as 24 h post-injury. The earliest
indication of the development of the pathological process in the lungs was the increase
and deformation of the pulmonary pattern in root segments as a result of vascular
hyperaemia, which was caused by hypertransfusion.
- Diagnostics of pulmonary complications (e.g., RDS, cardial
pulmonary oedema, and severe pneumonia in the pre-clinical period) was possible through
evaluation of the dynamics of the radiological changes. This allowed early adequate
intensive therapy.
- Respiratory distress syndrome and haemodynamic pulmonary
oedema detected in burn patients with IT did not have specific diagnostic features in this
group of patients compared with other patients with pulmonary complications. Most of the
difficulties arose in the diagnostics and differential diagnostics of RDS.
- Comparative analysis of clinical cases and data from animal
experimental studies showed the difference in radiological features, which depended on the
type of injury to the vascular pulmonary channel. This difference permitted differential
diagnostics between haemodynamic pulmonary oedema, RDS, and pneumonia. RDS was
characterized by diffuse strengthening and deformation of the pulmonary vascular pattern
and focal changes mostly located in the peripheral pulmonary fields. In cases of HPO the
presence of large central unstructured zones was typical.
RESUME. Les Auteurs
considèrent les brûlures légères avec un prognostic potentiellement favorable, dont
les effets ont été notamment aggravés par la présence de traumatismes causés par le
feu. Dans le groupe de patients pris en examen, les dix-sept fatalités prévues ont été
en réalité 27. Les investigations radiologiques ont fourni beaucoup d'informations très
importantes, parce qu'il était possible de prédire les complications polmonaires en
évaluant l'évolution de la dynamique des modifications radiologiques. En cette manière,
les premières phases de la thérapie intensive ont été facilitées.
BIBLIOGRAPHY
- Pruitt B.A., Flemma R.J., Di Vincenti F.C., Foley F.D.,
Mason A.D.: Pulmonary complications in burn patients: a comparative study of 697 patients.
J. Thorac. Cardiovasc. Surg., 59: 7-20, 1970.
Schatzki R.: Roentgenologic report of the pulmonary
lesions. Ann. Surg., 117: 841-64, 1947.
Pruitt B.A., Erickson DR., Morris A.: Progressive pulmonary
insufficiency and other pulmonary complications of thermal injury. J. Trauma, 15: 369-79,
1975.
Chi-Shing Chu: New concepts of pulmonary burn injury. J.
Trauma, 21: 958-61, 1981.
Horovitz, J.H.: Diagnostic tools for use in smoke
inhalation. J. Trauma, 21: 717-9, 1981.
Munster A.M.: The early management of thermal burns.
Surgery,88: 29-40, 1980.
Teixidor H.S., Rubin E., Novic G.S., Alonso D.R.: Smoke
inhalation: radiologic manifestations. Radiology, 149: 383-7, 1983.
Demling R.H.: Burns. N. Eng. J. Med., 313: 1389-98, 1985.
Edward F., Haponik M.D. et al.: Increased vascular pedical
width preceding burn-related pulmonary edema. Chest, 90: 681-5, 1986.
Herndom D.N. et al.: Pulmonary injury in burned patients.
Surg.Clin. N. Amer., 67: 31-46, 1987.
This paper was presented at the
Third International Conference on Burns and Fire Diasters
held in Palermo, Italy in June 1995.Address
correspondence to: Prof. O.D. Dmitrienko
Department of Radiology
St Petersburg Medical Academy of Postgraduate Studies
St Petersburg, Russia. |
|