| Annals of Burns and Fire Disasters - vol. X - n. 4 - December 1997
USE OF SOLCOSERYL IN MINOR BURNS
Ghoneimi I.G.(1), Bang R.L.(1,2) (1) Al-Babtain Centre for Plastic
Surgery and Burns, Kuwait SUMMARY. A study was made in Kuwait of forty minor burn patients treated as out-patients from February 1994 to April 1995 (27 males/13 females; mean age 19 yr ; age range 1-47 yr). Twenty-six patients sustained scalds, five flame burns, five contact burns, and four had electric flash burns, The extent of burn ranged from I to 12% total body surface, mainly involving the lower limbs. Thirty-eight patients sustained dermal burns and two had minimal full-thickness burns. The burn wounds were treated with topical Solcoseryl'.* Solcoseryl dressing was easy to use, comfortable, and well tolerated by the patients. The spontaneous wound heating in 7 to 29 days (mean 18 days) conformed to initially assessed burn depth in the majority of patients. The favourable healing showed that no post-injury deepening of the burn wound had occurred. The incidence of hypertrophic scarring was comparatively less in Solcoseryl-treated patients. Solcoseryl is therefore is a good topical agent for the management of minor burn wounds. Introduction The management of the burn wound is aimed
at prevention of infection and at the arrest of impending tissue necrosis, so that healing
ensues favourably in partial-thickness burns. Superficial partial-thickness burns heal
within two weeks without scarring, but deep partial-thickness burns are often problematic.
The problem is aggravated by the inherent tendency of these burns to deepen during the
first three days post-injury and become infected, developing hypertrophic scars. A healing
time extending beyond the third week postburn leads to abnormal scar formation. Wound
dressing plays an important role in burn patients in whom spontaneous healing is
anticipated. An ideal wound dressing should be easy to apply and remove, stay in place,
relieve pain, protect from infection, ntinitnize disruption of the wound bed, encourage
re-epithelialization, and be cost-effective. The search for an ideal dressing continues,
in burn wound care. Material and methods Forty minor burn patients who from
February 1994 to April 1995 attended Al-Babtain Centre for Plastic Surgery and Burns
(Kuwait) within 24 h post-burn were included in this study. The burn area was mapped out
according to the Lund and Browder chart. Burn depth was judged on the basis of various
clinical criteria. After initial burn wound swabs had been taken, the area was covered
with Solcoseryl and gauze and then bandaged. All patients were treated as out-patients.
The dressing was inspected every day and changed if needed - otherwise it was routinely
changed on alternate days until complete healing occurred. WouDd swabs were taken twice a
week as a part of microbial surveillance. Subjective comments of pain, ease, comfort and
tolerance of dressing, as well as objective assessment of the wound condition, swab
results and the healing process, were recorded twice a week until complete. Once the
wounds had healed, they were reviewed every month for a period of six months to assess
scar quality, and photographic records were taken. Results Twenty-seven male and thirteen female patients with a mean age of 19 yr (range 1-47) were studied (Table I).
Twenty-six patients sustained scalds, five flame burns, five contact burns, and four had electric flash burns. The extent of burn varied from <=1-12% total body surface area (TBSA), although the majority of patients sustained :<= 5% burns (Table II).
Thirty-eight patients presented dermal burns and two had full-thickness burns. In the patients who sustained full-thickness burns, the extent was less than 1 %. The body parts involved are depicted in Table III - the majority of patients (70%) sustained limb burns. Thirtyseven patients reported that use of Solcoseryl caused no pain and that it was quite a comfortable dressing, while three commented otherwise. The application and removal of Solcoseryl were easy - the dressing did not smell abnormal, and it was easy to observe the healing process. The wound swab results showed colonization of organisms in thirteen patients, but no clinical infection occurred in any of them. No allergic reaction occurred during the course of treatment.
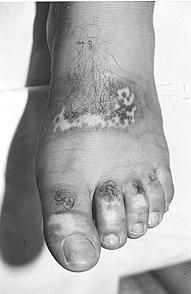
The burn areas healed completely (Table IV) in 7 to 29 days (mean, 18 days).
The superficial dermal burns (Fig. 1) healed in about 11 days, mixed dermal burns (Fig.2) in 19 days, and deep dermal and full-thickness burns (Fig. 3) in 23 days. Thirty-six patients had acceptable scars while four developed hypertrophic scars. Two patients who developed hypertrophic scars had full-thickness burns, which took more than three weeks to heal. Hypopigmentation was observed during follow-up in four patients, and hyperpigmentation in eight. There was no incidence of post-burn contracture and the scars remained stable in all the patients.
Discussion All wound care techniques require planned
regular dressing changes, although the interval may vary. Each area of the burn should be
washed and debrided thoroughly with each dressing change. It is comfortable for patients
if a topical agent can be applied and removed easily, causes no pain, is odour free, and
stays on for a long time: we found Solcoseryl altogether acceptable in this regard.
RESUME. Cette étude, effectuée en Kowéit, a pris en considération 40 patients avec des brûlures mineures traités en consultation externe dans la période février-avril 1995 (mâles/femelles, 27/13; âge moyen, 19 ans; limites d'âge, 1-47 ans). Vingt-six patients ont subi des ébouillantements, cinq des brûlures par flamme, cinq des brûlures par contact, et quatre des brûlures électriques. Le pourcentage de la surface brûlée variait de 1 à 12% de la surface corporelle totale, et intéressait principalement les membres inférieurs. Trente-huit patients ont subi des brûlures de la peau et deux présentaient des brûlures minimales à toute épaisseur. Les lésions des membres ont été traitées avec le Solcoseryl@.* La médication avec Solcoseryl était facile à appliquer, confortable et bien tolérée par les patients. La guérison spontanée de la lésion en 7 à 29 jours (moyen, 18 jours) était, dans la majorité des cas, en conformité avec la profondité de la brûlure évaluée initialement. La guérison favorable indiquait que les lésions n'étaient pas devenues plus profondes dans la période successive. Uincidence de la cicatrisation hypertrophique était mineure dans les patients traités avec le Solcoseryl. Les Auteurs concluent que le Solcoseryl est un bon agent topique pour le traitement des brûlures mineures. BIBLIOGRAPHY
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||