| Annals of Burns and Fire Disasters
- vol. X - n. 4 - December 1997
CHARACTERISTICS AND DYNAMICS OF THE PSYCHOLOGICAL
CONSEQUENCES IN CHILDREN SUFFERING THERMAL INJURY
Andreeva D., Atanasov A.
Siem Pirogov Centre for
Burns and Plastic Surgery, Sofia, Bulgaria
SUMMARY. A description is
given of the regular connection between thermal injury and its consequences (disability,
functional and cosmetic defects) and its reflections on child psychology - a high degree
of anxiety, an inferiority complex, neuropathic tendencies, negative self-acceptance, and
aggressive behaviour. The investigation concerned 217 cases of burn consequences among
children aged 3 to 18 years. The psychological methods used were: the
"Draw-a-person" and the "Bewitched Family" tests; the SCSA scale
(classical and sociosituational anxiety and agitation of mind); Dernbo-Ruben stain's
self-evaluation test; Eysenck questions; IQ test; test for degree of pretensions; and the
polyphase personal questionnaire.
Introduction
In the last
twenty years many Burns Centres have begun to use psychological rehabilitation as a
routine method in the overall complex of burns treatment. The application of this method
is motivated by the objective reality of post-burn consequences, which cause difficulties
for patients in their interpersonal social relations and adaptation.
Our activity at the Pirogov Centre for Burns and Plastic Surgery (Sofia, Bulgaria) is
orientated in two main directions: psychotherapy support during medical treatment, and
preparation for adaptation and social development.
While for adult patients with a normal level of intelligence the process of adaptation
proceeds fairly easily, in children - because of their undifferentiated nervous system,
their unstable and still improving psychological processes, and their poor personal
defences - burn treatment requires a close connection and interaction between the medical
team, the psychologist, the affected child, and the parents. Unexpected traumas, acute
pain, and sudden separation from the family following rapid hospitalization present the
young patient with urgent demands for adequate adaptation to a completely unknown and
exceptional situation, involving countless painful manipulations (infusions, dressing
changes, operations, etc.). These requirements for rapid adjustment of the dynamic
stereotype are a serious challenge to the adaptational mechanisms of the central nervous
system.
A specific peculiarity of burns is the double experience of the trauma - short in itself
but lasting from the time of the accident until convalescence - a prolonged process in
time and painful for the patient because of the consequences and complications of serious
burns, which often demand corrective operative interventions.
Purpose of the study
The purpose of the study
was to show and explain the natural connection between changes in the physical
"Me" and consequeDces in the adolescent mind - an inferiority complex, a high
degree of anxiety and neurotic symptoms, social passivity, and nonintegration.
Psychodiagnostic
methods
Objective
drawing tests - "Draw -a-person" (Machover) and the "Bewitched Family"
test (Kos and Borman). These give information about a person's degree of adaptability to
the external changes of the body, his/her way of interpreting the burn accident, and
conflicts and family relationships.
Self-evaluation test (D
embo -Ruben stain). This gives information about the level and the adequacy of the
person's self-estimation.
Test for degree of
pretensions. The purpose is to study the dynamics of the person's pretensions by means of
the gradation of various tasks of different difficulty which individuals set themselves.
SCSA scale (Kondash).
This scale concerns classic and sociosituational anxiety and agitation of the mind. It
determines the availability and the degree of a subjective, unpleasant feeling of
objective and situational fear that is provoked by objects of classic phobias,
sociointerpersonal situations, and the disturbance and emotions provoked by hospital
treatment.
QNTPD
(Questionnaire for neuroticism and tendentious personal deviations (Kokoshkarova) for the
screening of neurosis, offering the possibility for a syndrome estimation of the neurotic
disorder.
Eysetick's personal
questionnaire. This shows extraor introverted inner adjustment, emotional stability,
neuroticism, and peculiarities of temperament.
Polyphase personal
questionnaire for adolescents, including twelve spheres of manifestations in life: control
of impulses, emotional tone, body image, social relationships, morality, sexual
adjustment, family relationships, overcoming the external world, professional and
educational purposes, psychopathology, high degree of adaptation, idealism.
Lusher Test. This
considers emotional status and the presence of inner conflicts.
Raven's IQ test. This
measures the person's potential possibilities of intellectual development.
Altogether, 217
children aged 4 to 18 years were examined using the above tests. The results are divided
into the following groups:
Group 1: results in the
first month post-burn (independent of degree)
Group 2: results one
month post-burn, when it was necessary to perform face, neck and hand plastic surgery
Group 3: children
with post-operative sequelae
Group 4: children
suffering from severe cosmetic or functional sequelae in uncovered parts of the body and
from functional disability
Results
The projective
"Draw-a-person method" shows that children in Group I (one month post-burn) up
to the age of 12 years, although they had not entirely recovered from the thermal trauma,
quietly accepted their new physical 11 self-image", with hope and confidence that
"everything was OK". The interpretation of the accident in the "Bewitched
Family" drawing method showed that the child succeeded in avoiding the worst
consequences or suffered a temporary punishment. In children with fresh burns aged over 12
years - i.e, adolescents - the physical "self-image" was very much changed in
their ideas and was, for them, entirely unacceptable. This created great inner discomfort
and anxiety. The drawings of the "Bewitched Family" reflect family relationships
and conflicts when the child has at least a medial level of intelligence. This facilitates
the psychologists' work as regards the choice and application of psychotherapeutic methods
of influence, and can also orientate them when working with the child's parents.
QNTPD in children with fresh burns aged over 12 years showed that children with a
prolonged "bed regimen" were marked by certain neurotic tendencies to which the
psychotherapist had to pay special attention.
Self-estimation in children in this group was very close to adequate - it was reduced only
as regards the criterion "health", which is easy to explain. The pretension
level, when it was already formed (i.e. over the age of 7-8 years), was medial or slightly
increased.
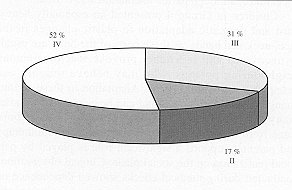
The SCSA scale showed that the level of anxiety increased in fresh burns (Tables I and
II). The scale was within normal limits in only 17 % of the children; in 31 % it
was third degree, and in 52% it was very high (fourth degree).
 |
 |
| Table
I - Results of SCSA in recent burns |
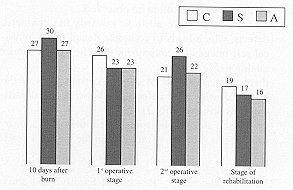
Table
II - Decreasing anxiety during treatment |
|
The qualitative estimation of the results
showed that the most recurrent fears were:
- Fear of bandages and operations
- Fear of a prolonged stay in hospital
- Fear of a sudden accident
Among children in Group 2
(plastic changes of the neck, face and hands after the fresh burn), the projective drawing
method showed complete denial of the physically changed "self-image" and a
confused secret hope that things would change for the better. The children experienced the
inner crisis of a split mind: on the one hand, they felt the same as before while, on the
other, they saw and understood the fact that they were not the same and that this change
was irreversible. Their drawings projected the search for support, understanding and
sympathy. Their self-evaluation was inadequate - self-esteem was either extremely low or
extremely high, which indicated that they had not succeeded in determining their place
among other children. Shy, unsure of themselves, and hypodepressive - these
characteristics were intensified by the need to wear elastic compression bandages for long
periods. Psychotherapeutic interviews with these children are very important;
collaboration with the parents is also of great significance, for they are the persons
from whom the child expects to receive unreserved love, support, understanding and
sympathy after discharge from hospital.
Results in Group 3 (consequences in covered parts of the
body) show that at the age of twelve years most of these children (about 67%) had adapted
well to their appearance, although partial adaptation also existed.
Children in Group 4 presented an especially heavy, hard and dramatic adaptation to plastic
changes in the face, neck and hands, as these parts of the body are usually uncovered and
inevitably provoke reactions among neighbouring persons, who may behave roughly and
indelicately or express regret. Adaptation to these serious changes is very prolonged and
can be achieved only after many operative corrections, especially when the burn dates from
early childhood. In addition to psychotherapy and parental support, a significant role is
played by personal realization on the social plane. Clinical observations conducted during
medical checks showed dependence on the degree of adaptation from the time of inclusion
and the adolescent's self-realization in socially significant relationships and
activities.
At adolescence three kinds of reactions
towards the changed appearance can often be observed:
- there is a negative attitude towards the
cosmetic defects, which leads to complete denial of the physical self-image and
consequently of the person's inner qualities (Fig. 1)
|
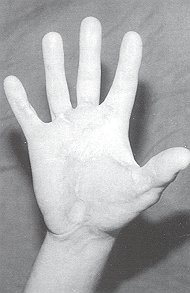
Fig.1
- Sixteen-year-old girl. Deep burn on palm
of right hand in early period post-burn.
Subjected to skin grafting. Mild contractive
and cosmetic defect. |
|
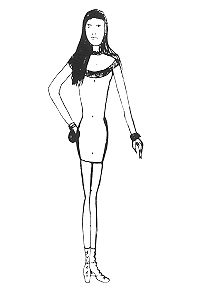
- there is non-acceptance only of certain
parts of the body, i.e. where the defect is; otherwise the identification is positive (Fig.
2)
|
Fig. 2 -
"Draw-a-person" test reflecting patient's image of her body. She tries to hide
defect |
|
- the person as a whole is integrated; the
outer appearance as it is, but this is reflected in the physical "selfimage" (Fig.
3)
The drawings in the "Bewitched
Family" test show that children from harmonious, complete and unite families adapted
more easily and quickly to the changed inner body image.

|
Fig. 3 - "Bewitched
Family" test: patient's drawing, indicating magician's goodness, reflects the
incapacity of her ego to give her a hand without defects. |
|
The self-estimation of
patients in Groups 3 and 4 did not indicate any statistically significant differences,
being changed and inadequate in both groups. Real self-esteem is the first indicator of
partial adaptation.
Examination of the degree of pretensions in Groups 3 and 4 shows that this was medial. A
failure was experienced as a collapse, reducing the level of pretensions by two or three
degrees. Contrarily, a success multiplied pretensions many times. This indicates an
instability of pretensions, which tend to reduce because of an unreal choice of purposes,
fear of failure, and caution.
The SCSA scale shows the following results in adolescents in Groups 3 and 4: boys, 67%,
scale indicated 2nd degree, and at 33% was increased, 3rd degree; girls, 2nd degree, scale
indicated 34.6%, increased 3rd degree at 38.4%, and 23% 4th degree - clearly increased (Table
III).
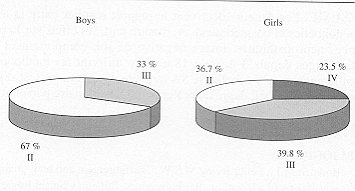 |
Table III - Results of SCSA by consequences |
|
The qualitative analysis
of the results shows however that even at a level of anxiety within normal limits, i.e.
2nd degree, there are high values as regards fear of social and interpersonal
communication. First place, with the greatest number of points, is fear of separation from
close relatives, followed in order by fear of being laughed at, fear of being ignored, and
fear of disapproval. While the fear of medical manipulations is predominant among children
with fresh sburns, among children with burn sequelae social and interpersonal contacts
cause the main fears - fears of how other people will accept and consider them. This to a
high degree motivates their desire for corrective treatment and explains the impatience
with which they expect results. The Polyphase Personal Questionnaire shows the
supersensitiveness of adolescents to their changed outer appearance and its reflection on
the regulation of their behaviour. Ninety-one per cent of the persons examined could not
tolerate criticism, and their feelings were easily affected. They were predisposed towards
revenge. They took serious care of their health, and their mental image of their future
appearance did not satisfy them. They considered themselves ugly and unattractive. About
77% confessed that it was extremely difficult for them to make friends. They were very
upset by other people's disapproval. They were undecisive and unsure of themselves in
their approach to the outside world, and afraid of the thought that one day they would be
grown up. They were afraid of the future in general and preferred not to think about it.
In all the patients the Lusher test showed a displacement of the basic necessities and
their compensatory replacement by secondary necessities - this is a manifestation of inner
conflict and is also a precondition for the development of neurosis.
The Eyselick questionnaires, QNTP1) and IQ tests help the psychologist to investigate the
patient's personal peculiarities and to choose adequate psychotherapeutic methods. In
practice, the most widely used techniques are the psychotherapeutic interview, games,
observation, cognitive methods, behavioural techniques, and autogenic training.
Conclusions
Burn sequelae naturally reflect on the
mind and on the mental regulation of behaviour and activity. These consequences create
barriers against communication and they hinder social adaptation and manifestation. By
means of a variety of psychotherapeutic methods, the psychologist endeavours to reduce the
patient's anxiety by removing neuroses, creating a positive adjustment to the changed
physical image, and stabilizing a feeling of self-importance and acceptability. Because of
corrective surgery's great influence on the patient's psychological status, surgeons have
to solve the problem of the permanent improvement offered by curative methods for the
treatment of sequelae.
RESUME. Les
Auteurs décrivent le rapport régulier entre la lésion thermique et ses conséquences,
d'une part (incapacité, insuffisances fonctionnelles et cosmétiques), et, d'autre part,
les effets sur la psychologie de l'enfant (haut niveau d'anxiété, complexe
d'infériorité, tendances neuropathiques, image négative de soi, comportement agressif).
Ils considčrent 217 cas de conséquences de brűlure chez des enfants âgés depuis 3
jusqu'ŕ 18 ans, en utilisant les méthodes d'observation psychologiques suivantes:
"dessinez une personne" ; "la famille enchantée"; échelle SCSA
(anxiété et agitation); test d'évaluation de soi selon Dembo-Rubenstain; questions de
Eysenck; test de quotient intellectuel; degré de prétention; questionnaire personnel
polyphasé.
BIBLIOGRAPHY
- Bowden M.L.,
Feller Irving M.S.W.: Disfigurement and body image as variables in adaptation after burn
injury. Bulletin Clinical Review Burn Injuries, Sept. 1982.
Kammerer B.: School re-entry program
for the burned child.Bulletin Clinical Review Burn Injuries, Sept. 1982.
Konigova R., Pondelieek L: Role of
"accompanying" relatives in burn care. Bulletin Clinical Review Burn Injuries,
Sept. 1982.
Levinson P., Onsterhout D.K.: Art and play
therapy with pediatric burn patients. J. Burn Care Rehabil., 9/10: 1980.
Gottsdanker R.: "Experimenting in
psychology". Prentice-Hall, Inc., Englewood Cliffs, New Jersey, 1982.
Walls D.:
Apre-operative play program for burned children. Bulletin Clinical Review Burn Injuries,
Sept. 1982.
| This
paper was received on 17 April 1997. Address correspondence to: Dr D. Andreeva and Dr N. Atanasov
Siern Pirogov Centre for Burns and Plastic Surgery
Sofia, Bulgaria. |
|