| Annals of Burns and Fire Disasters - vol. XI - n. 1 - March 1998
KERATINOCYTES AS BIOLOGICAL DRESSING IN
THE TREATMENT OF PARTIAL-THICKNESS BURNS IN CHIILDREN
Dédovic Z.*, Koupilovià I.**,
Suchànek V.*
*Burn Centre, Bohunice
Teaching Hospital, Masaryk University, Brno, Czech Republic
**Department of Social Medicine, Faculty of Medicine, Masaryk University, Brno
SUMMARY. In order to
evaluate the treatment of deep dermal burns with keratinocytes and to establish the
possibility of reducing hospitalization and the frequency of painful wound rebandaging, a
survey is presented of 109 children with deep dermal burns treated with cultured epidermal
allografts. The decline in the mean duration of hospitalization was statistically
significant compared with that of children treated without the use of keratinocytes. The
healing of deep dermal burns treated with keratinocytes was successful in all patients, in
accordance with our expectations. The application of these biological allografts had to be
repeated - twice at most - in only in 24.7% of cases.
Introduction
A retrospective review was made of all
children with partial-thickness burns admitted to the burn centre in Brno (Czech Republic)
from 1992 to 1995 and treated with cultured epidermal allografts. Since 1992 keratinocytes
have been used routinely as a biological dressing in the treatment of burn wounds. This
method of mobilizing the body's own healing potential for deep dermal burns has become an
important tool in the treatment of children's burns. As the treatment of full-thickness
burns with cultured epidermal allografts or autografts proved unsuccessful, we focused on
the use of keratinocytes in the treatment of partial-thickness burns only. In the period
in question, an annual average 125 children were hospitalized in our burn centre; 50% of
these were in the most vulnerable age group between 0 and 3 yr of age.

|
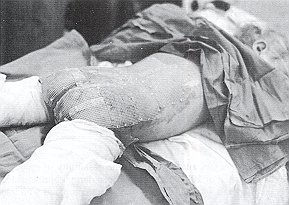
Fig. 1 -
Application of keratinocytes in partial-thickness burn. |
|
Almost 80% of the children hospitalized
were scalded. The aim of the present study was to evaluate the use of keratinocytes as a
biological dressing in order to reduce the period of hospitalization, especially that of
young children, who constitute a particularly traumatized group exposed to psychological
and physical stress in the event of prolonged hospitalization.
Patients and methods
From October 1992 to 31 December 1995
we hospitalized 109 burned children between 0 and 14 yr of age treated with cultured
epidermal allografts. We investigated separately children with deep dermal burns (Figs.
1, 2) and those with mixed burns (partial-thickness and full-thickness) (Figs.3,4).
The characteristics of these groups were compared with 60 children admitted to our Centre
in 199 1, when the method of keratinocyte treatment had not yet been introduced
 |
Fig. 2 -
Partial-thickness burn after removal of keratinocytes (same .patient as Fig. 1). |
 |
 |
| Fig. 3
- Application of keratinocytes in portion of partial-thickness burn in patient with
extensive mixed burns. |
Fig. 4 -
Healing of part of partial-thickness burn after removal of keratinocytes (same patient as Fig.
1). |
|
The preparation of keratinocytes was
performed according to standard routine and protocol. The most commonly used area for the
harvesting of viable keratinocytes is the skin of the posterior side of auricles obtained
during the surgical procedure of otoplasty in children aged 6 to 12 yr. The total
duration of the growth of cultured epidermal keratinocytes was most frequently 20
days. The culture was grown using a slightly modified Rheinwald-Green technique. The
cultured epidermal grafts were in the form of a multilayer of two to nine layers fixed on
to the carrier as a substitute for its own missing keratinocytes at the surface of
partial-thickness burns. The preparation of the wound bed for the application of
keratinocytes was of decisive importance for the outcome of the whole procedure. The wound
bed had to be clean, well vascularized, free from necrotic tissue residues, and with a
minimum of contamination. Because of this, keratinocyte treatment was started
comparatively late after the treatment with 1% silver sulphadiazine, which supported the
debridemerit and healed the surrounding superficial burns. After a 24 h intermission
without antiseptics or silver sulphadiazine, the wound bed was ready for keratinocyte
treatment. The dressing was changed for the first time 48 h after application of the
graft, when it had already adhered to the surface of the wound and the carrier was easy to
remove.
Results
The characteristics of patients
treated and not treated with cultured epidermal allografts can be seen in Table I. The
duration of hospitalization in patients with second-degree burns ranged from 7 to 37 days
in 1991 and from 6 to 30 days in 1992-95, respectively.
| |
1991
No grafts |
1992-95
Grafts |
| N' patients |
60 |
109 |
| Males (%) |
59.7 |
59.8 |
Partial - thickness burns (%)
(II degree) |
83.3 |
67.0 |
Partial - and full - thickness (%)
(II+III degree) |
16.7 |
33.0 |
|
| Table I - Characteristics of children treated and
not treated with cultured epidermal grafts |
|
The mean duration of
hospitalization was 17 days in 1991, dropping to 13.1 days in 1992-1995. The decline in
the mean length of hospitalization of patients with partial-thickness burns was almost
four days, which was statistically very significant (difference for 11 degree: 3.9 [95 %
Cl 2.0, 5.91 days =p < 0. 00 1) (Table II).
| |
1991
No grafts |
| II degree |
II+III degree |
|
1992-95
Grafts |
| II degree |
II+III degree |
|
| N' patients |
50 |
10 |
73 |
35 |
| Min. |
7 |
24 |
6 |
10 |
| Max. |
37 |
58 |
30 |
68 |
| Mean |
17.0 |
34.4 |
13.1 |
28.6 |
| S. |
6.8 |
10.2 |
4.0 |
12.5 |
| 95% CI |
/15.1, 19.0/ |
/27.1, 41.7/ |
/12.2, 14.0/ |
/24.3, 32.9/ |
|
| Table II - Length of hospitalization in days in
children treated and not treated with cultured epidermal grafts |
|
The length of hospitalization in patients
with mixed second- and third-degree burns ranged from 24 to 58 days in 1991 and from 10 to
68 days in 1992-95. The mean length of hospitalization dropped from 34.4 days in 1991 to
28.6 days in 1992-95, but the difference was not statistically significant (difference for
11 + III degree: 5.8 [95% Cl -2.9, 14.51 days p = 0.188). It should be noted that we
treated only the deep dermal portions of mixed burns.
Table III shows that the treatment of patients with cultured epidermal grafts from
1992 to 1995 was successful in all 73 children with partial-thickness burns only.
| Treated successfully |
II degree |
II+III
degree |
| Yes |
73 (100%) |
28 (77.8%) |
| No |
- |
8 |
| Total |
73 |
36 |
|
| Table III - Success of treatment in patients treated with
cultured epidermal grafts in 1992-95 |
|
The proportion of
successfully treated deep dermal burns in patients with partial- and full-thickness burns
was 77.8% in our sample. In eight patients with mixed burns, autografting had to be
performed in the area treated unsuccessfully with keratinocytes. This was due either to
erroneous estimation of burn depth or to possible contamination of the wound. In 24.7 % of
children with partial-thickness burns, application of keratinocytes was repeated twice at
most (Table IV). The difference in the proportion of autografts performed in
children with partial-thickness burns and in those with mixed burns was statistically
highly significant.
| |
II degree |
II+III
degree |
p value |
| N' patients |
73 |
26 |
|
| Autograftings |
0 |
27.8 |
< 0.001 |
| Repeated applications of
cultured epidermal grafts (%) |
24.7 |
41.7 |
0.069 |
|
| Table IV - Autograftings and repeated application of
cultured epidermal grafts according to diagnoses |
|
Table V shows
that the period of grafting ranged from 3 to 18 days in patients with partial-thickness
burns and from 4 to 28 days in those with mixed burns. The average period of grafting was
9.8 days in children with only partial-thickness burns and 13.2 days in those with mixed
burns. The grafting in patients with more complicated injuries (mixed burns) was thus
performed 3.4 days later on average, a difference that was statistically highly
significant (difference 3.4 [95% CI 1.9, 4.81 days p < 0.001).
| |
II degree |
II+III
degree |
| N° patients |
73 |
36 |
| Mean |
9.8 |
13.2 |
| S. |
3.2 |
4.4 |
| Min. |
3 |
4 |
| Max. |
18 |
28 |
| p25 |
8 |
10 |
| p50 |
9 |
13 |
| p75 |
12 |
15.5 |
|
| Table V - Days of grafting in children
treated with cultured epidermal grafts in 1992 to 1995 according to diagnoses |
|
The success of treatment in children
treated with keratinocytes according to the day of grafting is shown in Table VI.
Looking at the relationship between the time of grafting and the success of treatment in
the group of patients with mixed burns, we found in our sample that successful
keratinocyte treatment did not depend on the time of application. There was no
statistically significant difference in linear trend in the proportion of successfully
treated patients in the three categories of grafting time.
| Days |
12 |
12-14 |
15+ |
| Total |
10 |
13 |
13 |
| Successfully treated |
70.0 |
69.2 |
92.3 |
| Test for heterogeneity |
p = 0.288 2d.f |
|
|
| Test for linear trend |
p = 0.189 1 d.f |
|
|
|
Table VI -
Success of treatment in patients with 11 + III degree treated with cultured epidermal
grafts according to day of grafting |
|
Discussion
Keratinocytes isolated from small skin
biopsies and cultured according to the Rheinwald-Green technique' are able to undergo
rapid expansion in vitro and may be regarded as a form of biological dressing in deep
dermal burn.
The aim of our study was to determine the effectiveness of using keratinocytes in the
treatment of partial-thickness burns.' Keratinocyte treatment presents both advantages and
limitations in its use. Our results show that the treatment of children with partial
-thickness burns was relatively successful in our burn centre between 1992 and 1995. In
addition to other advantages of this particular treatment strategy, a significant decrease
was observed in the average length of hospitalization. The humaneness of this method also
consists in the immediate pain relief and the reduction in the number of painful wound
dressings, a matter of cardinal importance for children who are exposed to the extreme
physical suffering and psychic stress induced by hospitalization.9 In patients with both
partial and full-thickness burns keratinocyte treatment was successful in more than
three-quarters of our patients. The failure of the method in the other patients in this
group could well be explained by the immediate vicinity of full-thickness burns and
contaminated necrectomized areas.
With regard to limitations in their use, the application of keratinocytes is not suitable
in certain body areas. In our experience, the back, neck, and certain parts of the head
are not the preferred areas, because dressings in these body sectors are rather difficult
to apply and grafts are more susceptible to the mechanical loss of cultured human
keratinocytes than are routine autografts." The arms, legs and the anterior trunk are
preferable sites of coverage." Some authors recommend the application of splints for
limbs in patients with cultured epidermal grafts, thus avoiding pressure in the areas
treated. Silver-containing local antiseptics (sulphadiazine silver, silver nitrate) cause
moderate inhibition of growth. The cost of keratinocyte treatment is high but so far no
optimal, safe and inexpensive method of wound bed preparatioln and of healing deep dermal
burns has been found.
RESUME. Les
Auteurs, dans le but d'évaluer le traitement de brûlures thermiques profondes moyennant
les kératinocytes et de trouver des modalités pour abbrévier l'hospitalisation et
réduire le numéro des procédures douloureuses des médications, présentent les
résultats d'une étude sur 105 enfants brûlés atteints de brûlures dermiques profondes
traitées avec des allogreffes épideriniques cultivées. La réduction de la durée
moyenne de l'hospitalisation a été statistiquement significative par rapport au
traitement des enfants traités sans l'emploi des kératinocytes. La guérison des
brûlures dermiques profondes traitées avec les kératinocytes s'est démontrée un
succès dans tous les patients, selon les prévisions des Auteurs, et il a été
nécessaire de répéter l'application de ces allographes biologiques seulement dans 24,7
des cas.
BIBLIOGRAPHY
- Rheinwald J.G., Green H.: Serial cultivation of
strains of human epidermal keratinocytes: the formation of colonies from single cells.
Cell, 6: 331-44, 1975.
- Eldad A., Burt A., Clarke J.A.: Cultured
epithelium as a skin substitute. Burns, 13: 173-80, 1987.
- Van der Merwe A.E., Mattheyse F.J., Bedford M. et
al.: Allografted keratinocytes used to accelerate the treatment of burn wounds are
replaced by recipient cells. Burns, 16: 193-7, 1990.
- Brychta P., Suchdnek L, Rihovd H. et al.: Cultured
epidermal allografts for the treatment of deep dermal burns. Acta Chir. Plast., 37: 20-24,
1995.
- Still J.M., jr, Orlet H.K., Law E.J.: Use of
cultured epidermal autografts in the treatment of large burns. Burns, 20: 539-41, 1994.
- Compton C.C.: Current concepts in pediatric burn
care: the biology of cultured epithelial autografts: an eight-year study in pediatric burn
patients. Eur. J. Pediatric Surg., 2: 216-22, 1992.
- Fratianne R., Papay F., Housini L, Lang C. et al.:
Keratinocyte a]lografts accelerate healing of split-thickness donor sites; applications
for improved treatment of burns. J. Burn Care Rehabil., 14: 148-54, 1993.
- Zhao Y.B., Zhao X.F., Li A. et al.: Clinical
observations and methods for identifying the existence of cultured epidermal allografts.
Burns, 18: 4-8, 1992.
- Pye R.J.: Cultured keratinocytes as biological
wound dressings. Eye, 2: 172-8, 1988.
- Odessey R.: Multicenter experience with cultured
epidermal autografts for treatment of burns. J. Burn Care Rehabil., 13: 174-80, 1992.
- Haith L.R., jr, Patton M.L., Goldman W.T.:
Cultured epidermal autografts and the treatment of massive burn injury. J. Burn Care
Rehabil., 13: 142-6, 1992.
- Heimbach D.M.: A nonuser's question about cultured
epidermal autografts. J. Burn Care Rehabil., 13: 127-9, 1992.
- Weekley R., Klein R.: Clinical nursing experience
with cultured epidermal autografts. J. Burn Care Rehabil., 13: 138-41, 1992.
- Bolgiani A., Patino 0., Benaim F.: The use of
modified Thomas splint for a patient with cultured epidermal autografts. J. Burn Care
Rehabil., 14: 466-70, 1993.
- Teepe R.G., Kreis R.W., Koebrugge E.J. et al.: The
use of cultured autologous epidermis in the treatment of extensive burn. J. Trauma, 30:
269-75, 1990.
- Brychta P., Adler J., kihovd H. et al.: Cultured
skin cells for treatment of burns. Ann. Medit. Burns Club, 7: 206-8, 1994.
| This paper was received on 20 August
1997. Address correspondence to:
Dr Z. Dedovic Z.
Burn Centre, Bobunice Teaching Hospital, Masaryk University
Bmo, Czech Republic. |
|