Annals of Burns and Fire Disasters -
vol. XI - n. 2 - June 1998
EXPERIENCE OF
THE PLASTIC SURGERY AND BURNS DEPARTMENT OF THE GRIGORE ALEXANDRESCU CHILDREN'S CENTRAL
HOSPITAL (BUCHAREST) IN THE TREATMENT OF BURNED CHILDREN
Enescu
D., Enescu M., Stoicescu M., Voicu R.
Plastic
Surgery and Burns Department, Grigore Alexandrescu Children's Central Hospital, Bucharest,
Romania
SUMMARY. Before 1988 the care of burned children in Romania was in
the hands of generic burn specialists, and it was only in that year that a specialized
Burns and plastic surgery unit was established in the Children's Central Hospital in
Bucharest. This remains the only one in the country for the specialized treatment of
burned children, many of whom continue to be treated in unspecialized units. The results
of care of burned children have now significantly improved. The purpose of this
retrospective study is to report on the main epidemiological and clinical aspects in the
care of burned children in Romania and to suggest some therapeutic principles based on
practical experience. Early surgical management of the burned wound is recommended as the
most important therapy for improving survival after extensive burns.
Introduction
Until
1988 a few paediatric surgery departments, without any direct contribution from burn
specialists, provided empirical and fortuitous treatment for burned children in Romania.
In that year a plastic surgeon began to take care of burned children, and a Burns and
Plastic Surgery Unit was established in the Children's Central Hospital in Bucharest. This
department is still the only one in the country specialized in Burns treatment, and many
patients are admitted to other unspecialized units.
Our department is part of a University Emergency Hospital and has 32 beds. The staff is
composed of a plastic surgeon, an anaesthesiologist, a paediatrician and ten nurses
specially trained in Burns care (Fig. 1). Despite the poor material conditions, the care
of burned children has improved significantly every year.
The
purpose of this retrospective study is to reveal the main epidemiological and clinical
aspects and to suggest some therapeutic principles based upon experience.
Between 1988 and August 1997, some 7000 children were admitted to our Plastic Surgery
Department with Burn injuries of various kinds. We chose two groups of children (periods
1988-92 and 1992-96) and analysed the epidemiological and clinical issues related to age,
sex, aetiological agent, Burn surface, Burn depth, survival, complications and mortality
in relation to the extent of Burns and therapeutical methods.
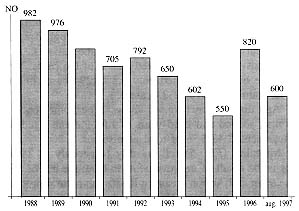
In 1997 the number of admissions dropped slightly (Fig. 2).
 |
 |
| Fig. 1 - The Bucharest Burns Centre for Children
Centre. |
Fig. 2 - Number of burned children admitted (7000). |
|
Hospitalization
was effected on the basis of the gravity standards of the ABA injury grading system. Minor
burns were treated on an out-patient basis. The criteria for the severity of the cases
admitted were TBSA, Burn depth, aetiological agents, anatomical distribution, age, and the
biological and social status of the patients. The high number of admissions is linked to
the high rate of burns among children in Romania - sometimes a single Burn unit is
insufficient. We realize that in 1996 the number of admissions increased because our unit
had become better known and its availability had increased.
|
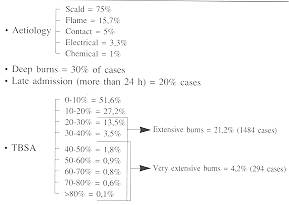
Fig. 3 Aetiology of burns. |
|
Fig.3
shows the high incidence of scald burns, especially in the youngest age group (0-3 yr).
Most scald Burns occurred in the home, during the preparation of rineals, as a consequence
of lack of supervision and care in the handling of hot liquids. Most of the accidents
could have been prevented. Although we had some doubts about the poor nutritional status
of the patients and the parents' psychological profile, we could not prove any cases of
child abuse.
 |
 |
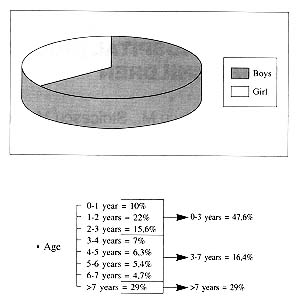
| Fig. 4 - Burn area in patients. |
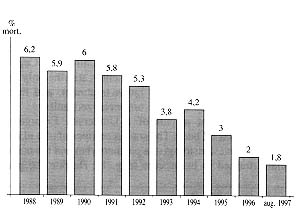
Fig. 5 - Mortality
rate |
|
Burns
affecting 0-10 % body surface area constituted the most frequent cases that we admitted.
The criteria for the admission of these cases were the aetiological agent, anatomical
distribution, and the age of the patients.
Extensive burns represented 21.2% of the cases. Very extensive burns constituted only 4.2%
(294 cases in nine yr, an annual average of 23 cases).
Age distribution (Fig. 4) shows a peak incidence in the first, second and third years of
life. Patients aged 0-3 yr represented 47,6 % of total admissions.
Mortality (Fig. 5) fell steadily (especially in 1996). This is the result of improvements
in care: the use of SSD 1% cream and Armon cream (a Romanian natural product) as topical
agents since 1992, early surgical management of the Burn wound, new classes of
antibiotics, and better methods of intensive care therapy.
In 1995-96, among children over seven years old, the mortality rate increased compared
with 1988-1993. This is without medical importance, since the overall mortality rate
decreased by more than half (Fig. 6).
Fig. 7 shows that in burns of less than 30% survival was 100% in 1996 and that in burns of
over 30% the expectation of survival increased, which is an excellent result for us
compared with the period 1988-1992. The good level of our results was due to our use of
clorhexidine solution, SSD and Armon for the prevention of infection.
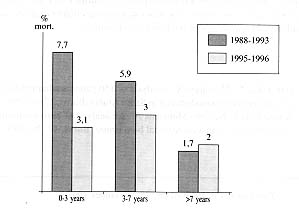 |
Fig. 6 - Mortality rate by age. |
|
The
data we present, as we know, are by no means new as regards the care of burned patients
but they confirm well-known epidemiological aspects and their
| |
1988-1992 |
1996 |
| TBSA |
% Survival |
% Survival |
| 1-9% |
100% |
100% |
| 10-19% |
98.8% |
100% |
| 20-29% |
91% |
100% |
| 30-39% |
68% |
80% |
| 40-49% |
49% |
80% |
| 50-59% |
28% |
67% |
| 60-69% |
18% |
50% |
| 70-79% |
17% |
60% |
| 80-89% |
10% |
- |
| 90-100% |
0% |
0% |
|
Fig. 7 - Survival rate in relation to TBSA. |
|
relative
stability. Our Unit endeavours to achieve good results in burn care despite somewhat poor
conditions compared with specialized centres in other parts of the world.
The results of the last years have rewarded our work in the care of burned children and
encouraged us to formulate some therapeutically principles, which we would like to
discuss. Early fluid resuscitation (Fig. 8) is available, starting from relatively small
Burn areas (less than 10%). With regard to fluid resuscitation, since 1992 we have used
the Carvajal formula. This formula has proved to be more efficient in children aged less
than 5 yr, providing good electrolyte balance and no renal failure. In Burn patients under
the age of 4 yr, the most frequent complications were sepsis , Burn encephalopathy and
digestive disorders (early metabolic and later septic). Early surgical management of the
Burn wound - primary and sequential excision followed by grafting - is the most important
therapy for improving the survival in extensive Burns, decreasing the incidence of sepsis,
reducing the cost and the duration of hospitalization, and improving the final functional
and aesthetic results. Man limited burned surfaces, which can be excised and grafted
early, are still treated by conservative measures until the formation of a granulating
wound. This is due to the parents' the radical refusal of early surgery.
In extensive Burns aggressive early excision and grafting can in many cases be
life-saving.
The successful cases that have we managed by means of surgical excision justify our hopes
that before long we we may accede to a skin bank.
The care of burned children is a complex medical activity that involves high costs and
requires the cooperation of a close-knit therapeutically team.
RESUME.
Avant 1988, la th�rapie des enfants br�l�s en Roumanie �tait confi�e � des
sp�cialistes g�n�riques des br�lures et seulement dans cette ann�e une unit�
sp�cialis�e pour la chirurgie plastique et la th�rapie des br�lures a �t� cr��e �
l'H�pital Central des Enfants � Bucarest. Cette unit� continue � �tre le seul centre
dans le pays pour le traitement sp�cialis� des patients p�diatriques br�l�s, dont un
grand nombre sont trait�s dans des centres non sp�cialis�s. Les r�sultats de la
th�rapie des enfants br�l�s s'est am�lior�e en mani�re significative.
Le but de cette �tude r�trospective est de pr�senter les aspects principaux
�pid�miologiques et cliniques des soins des enfants br�l�s et de sugg�rer des
principes th�rapeutiques bas�s sur des exp�riences pratiques. La gestion pr�coce
chirurgicale de la br�lure est recommand�e comme la th�rapie la plus importante pour
am�liorer la survie apr�s les br�lures �tendues.
BIBLIOGRAPHY
- Carvajal
M.F., Parks D.H.: Burns in Children, Chicago Year Book, Medical
Publishers, 1988.
- Ryan
C.A., Shankowsky H.A., Tredget E.E.: Profile of the paediatric Burn patient in a Canadian
Burn centre. Burns, 18: 267, 1992.
- Renz
B.M., Sherman R.: The Burn unit experience at Grady Memoral Hospital: 844 cases. J. Burn
Care Rehabil., 13: 425, 1992.
- Boswick
J.A., jr.: "The Art and Science of Burn Care". New York, Aspen,1987.
- Gupta
M., Gupta O.K., Goil P.: Paediatric Burns in Jaipur, India: An epidemiological study.
Burns, 18: 63, 1992.
- Lari
AR.A., Bang R.L., Ebrahim M.K.H.: An analysis of childhood burns in Kuwait. Burns, 18:
224, 1992.
- Danaf
A.E.l., Alashalash S.: Analysis of 150 patients admitted over a 2-year period to a modem
unit in Saudi Arabia. Burns, 17: 62,199 1.
- Benito-Ruiz
J., Navarro-Monzonis A.: An analysis of Burn mortality - A report from a Spanish regional
Burn centre. Burns, 17: 201, 1991.
| This paper was
received on 28 November 1997. Address correspondence to: Dr Dan Enescu, Plastic Surgery
and Burns Department, Grigore Alexandrescu Children's Central Hospital, Bucharest,
Romania. |
THE INTERNATIONAL FEDERATION OF SURGICAL COLLEGES
INVITES APPLICATIONS FOR 1998 TRAVEL GRANTS AND SURGICAL SCHOLARSHIPS
One of the principal aims of
the International Federation of Surgical Colleges is to provide international educational
opportunities and training programs for promising surgeons especially from the developing
countries. The Federation offers four Travel Grants annually through its own funds, and
provides other Scholarships through its Affiliates. A) Travel Grants are open only to
young medical graduates and surgical residents from the developing world who have
completed local training programs. The Grant is primarily for the purpose of promoting
worthwhile contacts and scientific exchanges by attending a major surgical meeting of the
candidate's choice (see list below), but it is hoped that the grantee will also take the
opportunity of visiting other surgical centers in the country where the scientific meeting
is being held. Each Grant will not exceed US$ 4,000, seen mainly as a contribution towards
travel, hotel and living costs during the meeting. It is to be noted that the Grant does
not guarantee total coverage of these costs and any excess must be met by the grantee. On
his/her return home the successful candidate will be expected to make a written report to
the IFSC. Application forms can be obtained from the address below. They must be completed
in full and returned, together with the required letters of sponsorship, to the IFSC, to
arrive not later March 31, 1998. Surgical scientific meetings taking place in 1998 are: 1.
Royal Australasian College of Surgeons Annual Scientific Congress, May 1998; 2. Royal
College of Surgeons of Edinburgh, Clinical and Scientific Meeting, May 1998; 3.
Mediterranean Club for Burns and Fire Disasters and IFSC Meeting, September 1998, Italy;
4. American College of Surgeons Annual Clinical Congress, October 1998, USA. B) The
Federation is also proud of being in a position to offer Scholarships through the
generosity of its affiliated Member organi the IFSC News or write to the Federation's
office, as below. Such scholarship are available in conjunction with the: 1. American
College of Surgeons; 2. Deutsche
Gesellschaft fijr Chirurgie; 3. Mediterranean
Club for Burns and Fire Disasters. Write or fax now to: The Secretary General,
International Federation of Surgical Colleges, Hospital of the University of Pennsylvania,
Department of Surgery - 4 Silverstein, 3400 Spruce Street, Philadelphia, PA 19104, USA,
Tel.: + 215 662-2024 - Fax: + 215 349-5849 - E-Mail: muldoon@maii.med.upenn.edu This is a
service to deserving surgeons in the developing countries. The Mediterranean Club for
Burns and Fire Disasters is a Member of the International Federation of Surgical
Colleges.zations. |
|