| Annals
of Burns and Fire Disasters - vol. XI - n. 2 - June 1998
CLINICAL AND STATISTICAL DATA ON THE OCCURRENCE
OF PULMONARY COMPLICATIONS IN SEVERE BURN PATIENTS TREATED IN AN INTENSIVE CARE UNIT
Belba M., Pema L., Dauti L, Mingomataj L, Isaraj S.,
Belba G.
Clinic of Burns and Plastic Surgery, University
Centre Hospital, Tirana, Albania
SUMMARY. burns
continue to be a seriously dangerous illness with a strong potentiality of a fatal
outcome, despite the intensive propaganda aimed at their prevention and the great steps
taken in the field of scientific treatment. One of the possible complications of the
course of the illness is pulmonary disease. The problem is focused on in this paper, which
provides a full epidemiological view of the complication seen in its different aspects. A
detailed analysis of the results of our work in the intensive care unit over a threeyear
period of time and the discussion of cases in accordance with the data in the Tables highlight
the age-groups most afflicted, the time of appearance of the complication, and the
interrelations between cause of burn, extent of burn, and death rate.
Introduction
The treatment of severely burned patients
is complex and difficult. The medical staff has to face very severe situations before the
condition gradually ameliorates. One important problem that appears during the course of
the disease is that of pulmonary complications. Prevention is possible but in most cases
it is the causative agent of the burn itself that conditions their development. Even when
the causative agent does not act directly on the respiratory tract the pathophysiology of
the burn injury presupposes the occurrence of pulmonary complications that may have
dangerous consequences as regards general prognosis.
Pulmonary complications may occur in the early acute post-burn and as well as in the later
period because of the prolonged profound catabolic state of the patient
A number of factors - familiarity with the burn disease, the taking of a detailed history,
a careful physical examination, a careful check of laboratory data, monitoring of the
patient and the follow-up - all help to estimate and predict the possible occurrence of
pulmonary complications, which are justifiably considered to be one of the main causes of
death in the severely burned patient.
The aim of this clinical and statistical survey was to provide data on the results of work
in our intensive care unit (ICU) in a three-year period of treating burned patients with
pulmonary complications.
Materials, methods and results
This paper presents an epidemiological and
clinical report on 97 cases treated in the ICU at the burns and Plastic Surgery Clinic of
the University Centre Hospital, Tirana, in the period January 1993-January 1996. All the
patients considered developed pulmonary complications.
Patients treated in the ICU fulfilled the following criteria:
- Adults with 111-degree burns in more than 15% BSA Adults
with 11-degree burns in more than 20% BSA
- Children with deep 11-degree or 111-degree burns in more
than 10% BSA
- Burns of the respiratory tract, chemical and electrical
burns, involvement of critical areas of the body in the elderly or in early infancy,
whatever the percentage
The amount of fluids to be given in the
first 48 h was determined according to the Parkland formula .4, ' The diagnosis of a
pulmonary complication was made on the basis of clinical, laboratory and X-ray
examination. In this paper we analyse the incidence of pulmonary complications, the age
groups of the patients, the time of appearance of complications, the different kinds of
pulmonary complications according to age group, the relationship with the extent of the
burn and the burning agent, the death rate, the causes of death, and the mean duration of
ICU hospitalization.
The results of the study are shown in the Tables.
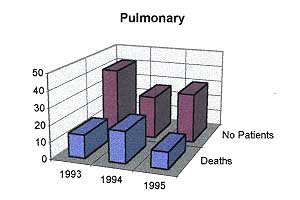
The study reveals that the presence of a pulmonary complication in a severely burned
patient had a generally constant occurrence rate, which varied from year to year but was
present in approximately one in five patients. Table I shows the cases with
pulmonary complications and the relevant percentages in successive years.
 |
Table 1 -
Frequency of pulmonary complications and the relevant percentages for each year |
| Year |
Number
of patients |
Pulmonary
complications |
| 1993 |
142 |
41 (29%) |
| 1994 |
117 |
26 (22%) |
| 1995 |
170 |
30 (18%) |
| Total |
429 |
97 (22%) |
|
|
Regarding the age groups (Table II), children
constituted 50 cases (51%), adults 38 cases (40%), and elderly patients 9 cases (9%). The
prevalence of children is explained by the fact that more than half of the patients
admitted to our ICU during this period were paediatric cases. Adults rather than children
were prone to pulmonary complications (28% and 19%, respectively), as seen if we analyse
the total number of patients according to age group.
 |
Table II -
Grouping of patients according to age (numbers in parentheses refer to pulmonary
complications) |
 |
 |
| Years |
Children
(<14 yr) |
Adults |
Elderly
(>60 yr) |
Total |
| 1993 |
85 (25) |
48 (11) |
9 (5) |
142 (41) |
| 1994 |
65 (13) |
43 (11) |
9 (2) |
147 (26) |
| 1995 |
113 (12) |
44 (16) |
13 (2) |
170 (30) |
| Total |
263 (50) |
135 (38) |
31 (9) |
429 (27) |
|
|
Table III, showing the time of
development of pulmonary complications, indicates that 32, i.e. one-third of the cases,
occurred within the first 48 h post-burn. Respiratory failure predominated in the early
post-burn period, generally in severe flame burns. The other 65 cases (two-thirds)
occurred after more than 48 h, corresponding to the septic phase of disease. The
complications in this phase were mainly acute pulmonary oedema, ARDS, bronchopneumonia and
pleurisy.
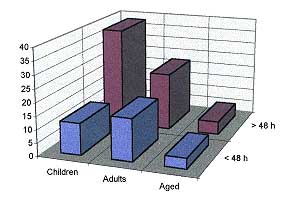 |
Table III
- Presentation of pulmonary complications according to time of appearance |
Years |
Children
(< 14 yr) |
Adults |
Elderly
(>60 yr) |
Total |
Early complications <48h |
12 |
16 |
4 |
32 |
Late complications >48 h |
38 |
22 |
5 |
65 |
Total |
50 |
38 |
9 |
97 |
|
|
Table IV shows
the pulmonary complications in relation to age and overall mortality. Diffuse bronchitis
had the highest incidence in children (19 cases, 5 deaths). Unilateral bronchopneumonia
occurred in 13 cases (2 deaths), and respiratory failure developed in 12 adults (11
deaths). Other types of pulmonary complications had an insignificant occurrence rate but
they must be taken into consideration in specific cases during treatment.
Age
group/
pulmonary pathology |
Children/
Deaths |
Adults/
Deaths |
Elderly/
Deaths |
Total/
Deaths |
Bronchitis |
19 / 5 |
5 / 1 |
- |
24 / 6 |
Unilateral |
13 / 2 |
5 / 2 |
2/ 1 |
20 / 5 |
bronchopneumonia
Bilateral |
6 / 3 |
1 / 0 |
2/ 1 |
9/ 4 |
bronchopneumonia
Pneumonia |
2 / 0 |
- |
- |
2/ 0 |
Pleuropneumonia |
1 / 0 |
- |
- |
1 / 0 |
Pleurisy |
3 / 1 |
5 / 1 |
1 / 1 |
9 / 3 |
EPA |
2 / 2 |
5 / 5 |
1 / 1 |
8 / 8 |
ARDS |
- |
3 / 3 |
- |
3 / 3 |
Pneumothorax |
1/0 |
2 / 0 |
- |
3 / 3 |
Respir.
insufficiency |
3 /2 |
12/11 |
3 /1 |
18 / 14 |
Total |
50 / 15 |
38 / 23 |
9 / 5 |
97 / 43 |
|
| Table IV - Nature of pulmonary pathologies
according to age |
|
Referring to Table
V, we notice that pulmonary complications generally developed in burns involving 2040%
BSA and nearly always in flame burns in more than 50% BSA.
Cause |
Flame |
Hot |
Hot |
Electric |
Chemical |
Total |
Surface % |
Respir |
No respir. |
water |
liquid |
burn |
burn |
deaths |
0<10% |
I / I |
I / 1 |
1/0 |
1/0 |
1/0 |
1/0 |
6/ 2 |
11 <20% |
2/0 |
6 /3 |
13 /0 |
7/0 |
1/0 |
1 / 1 |
30 /4 |
21<30% |
1 / 1 |
9 / 3 |
4/1 |
8 /2 |
1/0 |
- |
23 /7 |
31<40% |
2/2 |
1 /0 |
4/2 |
3 /2 |
- |
2/1 |
12/7 |
41<50% |
3 / 3 |
- |
- |
- |
- |
1/0 |
4 /3 |
51<100% |
21/19 |
- |
- |
- |
- |
1 / 1 |
22/20 |
Total |
30 /26 |
17/7 |
22 /3 |
19/4 |
3 /0 |
6 /0 |
97 /43 |
|
| Table V - Relationship of pulmonary complications
to burned BSA and cause of burn (numbers in parentheses refer to pulmonary complications) |
|
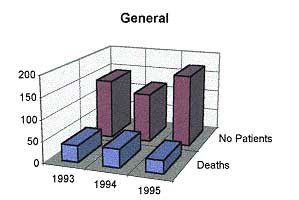
The overall death rate (Table
VI) for the three-year period of study was 26.3%. This rate reached 44.3% (43 deaths
in 97 cases) in patients developing a pulmonary complication.
 |
 |
| Year |
Number
of patients |
Deaths |
Pulmonary
complications |
Deaths |
| 1993 |
142 |
39 |
41 |
14 |
| 1994 |
117 |
43 |
26 |
19 |
| 1995 |
170 |
30 |
30 |
10 |
| Total |
429 |
112 |
97 |
43 |
|
| Table
VI - General mortality and mortality in cases with pulmonary complications |
|
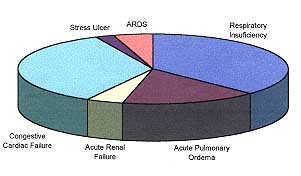
The causes of death (Table VII) were
respiratory failure (16 cases, out of 26 patients with airway burns), septic shock and
congestive heart failure (15 cases), acute pulmonary oedema (7 cases), and others.
|
Table VII
- Causes of death |
Causes |
Number
of deaths |
Respiratory
insufficiency |
16 |
Acute
pulmonary oedema |
7 |
Acute renal
failure |
2 |
Congestive
cardiac failure |
15 |
Stress ulcer |
1 |
ARDS |
2 |
Total |
43 |
|
|
The mean hospital stay of a patients
admitted to the ICU who developed a pulmonary complication was 11-20 days (Table VIII).
The short hospital stay corresponds to thecourse and prognosis of the patients, and
falls into two categories. The first category represents patients who successfully faced
complications and quickly recovered, while the second category corresponds to patients
with sepsis or airway burns, who died within an even shorter time.
 |
Table VIII - Mean
hospital stay in insensitive care unit |
| Year |
Mean hospital stay (days) |
| 1993 |
20 |
| 1994 |
11.3 |
| 1995 |
15 |
|
|
Discussion
Our statistical data confirm the
possibility of the occurrence of pulmonary complications in a severely burned patient, and
their increasing incidence. This is related not only to the increasing number of patients
who on admission present damage to the airways but also to the onset of a pulmonary
complication during the prolonged course of the disease in a septic patient.
In our data, the death rate of patients who developed a pulmonary complication was 1.6
times that of other burned patients. Of the 112 patients who had a fatal outcome in the
three-year study period, 43 (38.4%) died because of the severity of irreversibility of a
pulmonary complication.
Although most of our patients with pulmonary complications were children, adults were also
liable. The reason is that burns of the airways or extensive burns are more common in
adults than in children. The onset of respiratory failure during the period of burn shock
was the main cause of death in this category of patients.
Diffuse bronchitis and bronchopneumonia must be considered contributory complications of
burn sepsis in children.' Mortality due to these complications requires the utmost
attention, because the application of an appropriate resuscitation regimen, including
vigorous antimicrobial therapy, cart considerably reduce the danger they pose to the life
of a burned child. Cases with a fatal outcome generally correspond to patients who arrived
late at the burn centre or were not properly treated in the initial phases, and who in
addition to the complexity of their condition also suffered from a pulmonary problem.
Other pulmonary complications such as pneumonia, pleurisy and pleuropneumonia are uncommon
but cannot be disregarded, as they may be fatal. Pulmonary complications were present in
almost half of our elderly patients, uniformly distributed and without any special
features. In an elderly patient, clearly, careful account must be taken of the
circumstances of the burn accident, the history of any past or present disease, the
present general condition, the immunological state, age, etc.The triad composed of cause
of burn, extent of burn, and mortality is certainly the one that best explains their
interrelationships which may eventually may lead to pulmonary involvement.
The death rate was clearly higher in flame burns, in burns covering more than 50% BSA, and
above all in burns of the airways. When the burn agent did not directly damage the
airways, and also in scald burns, pulmonary complications appeared during the septic
phase, were less common, and had a better prognosis. Table V shows zero mortality
in electrical burns. The explanation of this finding is meaningful and is related to early
surgical treatment in these cases. Radical excisions and amputation of the limb involved
prevent the development of sepsis and consequently reduce the possibility of pulmonary
complications. In the absence of direct damage to the respiratory tract, the prevention of
pulmonary complications can be achieved only after early excision of the burn eschar,
which immediately eliminates dead tissue, thus obviating burn sepsis and its undesirable
consequences. Although without statistical substantiation, this is in fact our main
conclusion. In the presence of respiratory damage, strong automatic respiratory
support, in addition to supplementary therapy, is the only irreplaceable way to help face
the situation.
RESUME. Les brûlures
continuent à être une maladie grave et dangereuse qui peut facilement porter à la mort,
malgré les campagnes de propagande pour leur prévention et les progrès réalisés dans
le secteur de leur traitement scientifique. Une possible complication des brûlures
consiste en la maladie pulmonaire. Ce problème est considéré par les Auteurs, qui
présentent une vision épidémiologique complète de cette complication. Une analyse
détaillée des résultats de leur travail dans un centre de soins intensifs pendant une
période de trois ans et une discussion des cas sur la base des données présentées dans
les Tableaux soulignent les groupes d'âge les plus atteints, le temps du
commencement de la complication, et les rapports entre la cause de la brûlure, son
extension, et le taux de mortalité.
BIBLIOGRAPHY
- Dressier D.P., Hozid J.L., Nathan P.: "Thermal
Injury", St Louis, Washington DC, Toronto, 1988.
- Santos Heredero F.X et al.: Risk factors in the critical
burn patient. Ann. Medit. Burns Club, 3: 160-5, 1990.
- Mariscal-Sistiaga F. et al.: Azthreonam in the treatment of
pneumonia in major burn patients: A preliminary study. Ann. Medit. Burns Club, 6: 94-7,
1993.
- Baxter C.R. et al.: Guidelines for fluid resuscitation. J.
Trauma (suppl.), 21: 687, 1981
- Reaves L.E. et al.: Fluid and electrolyte resuscitation of
the thermally injured patient. World J. Surg., 7: 566-72, 1983.
- Masellis M., D'Arpa N., Napoli B.: Considerations on
intensive care in elderly burn patients. Ann. Burns Fire Disasters, 8: 207-213, 1995
- Mazzolini F. Therapeutic priorities in fire disaster. Ann.
Medit. Burns Club, 1: 152-9, 1988.
- Pettersen S.R., Umobred E., Warden G.D et a].: The
incidence of bacteremia following burn wound excision. J. Trauma, 22: 274,1982.
- Libber S.M., Staylon D.J.: Childhood burns reconsidered:
the child, the family and the burn injury. Trauma, 24: 245, 1984.
| This paper was received on 27
February 1997. Address correspondence
to: Dr Monika Belba
Clinic of Burns and Plastic Surgery
University Centre Hospital
Tirana, Albania. |
|