| Annals of Burns and Fire Disasters - vol. XI - n. 3 - September
1998
CRITERIA
FOR PATIENTS AT RISK IN RELATION TO MULTIORGANIC DEFICIENCY DUE TO BURN INJURIES
Yonov Y., Petkov P., Serdev N.
N.I. Pirogov Emergency Institute, Sofia,
Bulgaria
SUMMARY. A
prospective study was made of 700 burned patients treated at the Clinic of Thermal Trauma
in the N.I. Pirogov Institute, Sofia, over a 34-month period. Of these, 140 presented
moderately heavy and heavy Burns. Multiple organ failure (MOF) syndrome was found in 61
cases (43.57%). The criteria for assessing single-organ failure were those adopted in
world practice. If at least two organ functions proved to be critically disturbed we
considered that the patients had MOF syndrome. Patients with MOF were divided into two
groups: Group A (recovered - 15 patients) and Group B (deceased - 46 patients). A third
control group (Group C) comprised 20 patients with Burns of similar gravity, without MOF,
all of whom recovered. A statistical analysis was performed. The contingent at risk for
development of MOF consisted of: 1) male patients up to 50 years old and female patients
over that age; 2) patients with burns of the upper airways, Burns in over 30% TBSA, and
deep burns in over 10% TBSA; and 3) patients who developed sepsis or pneumonia.
Introduction
The notion of "sequential system
failure" as a synonym of "multiple organ failure" (M017) was introduced by
Baue in 1975. Previous reports on post-operative organ deficiency treated each organ
system as an isolated unit. Later studies established that multiple deficiency was
observed more often than single-organ failure and that its onset was either sudden or
gradual.
Since the beginning of the 1970s emergency medicine has been considered to be an
independent discipline, and researchers have started to analyse the prognoses of different
trauma outcomes. The probable course and outcome of the disease mainly depend on the
following factors:
- total burn area
- surface area of full-thickness burns
- localization of Burns
- age of patient
- time interval between moment of accident and initiation of
care
In all the patients in the series there
was a time lapse of 30 ± 5 min prior to commencement of care. The more serious the
trauma, the greater was the probability of the development of MOF. It was found that, in
similar types of burn, some patients recovered while others developed MOF and either only
survived with difficulty or died.
The aim of the present study was to establish what factors, in association with the
severity of burns, led to the development of the MOF syndrome, and to determine the groups
of patients at risk. A number of tasks were accomplished in order to achieve this aim: a
prospective study of the largest possible contingent of moderately severe and severe
burns, together with an analysis of cases in which MOF developed, plus a study of organic
complications in burn patients that could be regarded as risk factors for the development
of M0F.
Materials and methods
A prospective study was made of all Burn
patients (700) admitted to the Clinic of Thermal Trauma at the N.I. Pirogov Institute,
Sofia, in a 34-month period. The diagnosis of organ failure was based on
pathophysiological data in accordance with universally recognized medical criteria.
Cases of two or more organ deficiencies were defined as multiple organ failure syndrome.
We analysed deficiencies in eight functional systems of vital importance: 1. respiratory
system; 2. cardiovascular system; 3. secretory system; 4. gastrointestinal system; 5.
liver system; 6. endocrine system; 7. haematopoietic system; 8. immune system and central
nerve system following deficiency of liver detoxification function.
Treatment followed the therapeutic scheme adopted at our Clinic. Surgical interventions
were performed after spontaneous or accelerated elimination of necroses through chemical
or enzyme necrectorny or partial blood necrectomy. A control group of twenty patients was
observed, consisting of cases of burns of similar severity that did not develop the MOF
syndrome. Twenty supplementary factors were analysed that had some relation to the
development of MOF, such as factors linked to the course of the disease (e.g., onset of
organic deficiencies and bacteriological complications).
The data were processed using the W.J. Dixon Biomedical Computer Programs, 1989,
University of California.
Results
Over a period of almost three years (1
January 198730 October 1989), we observed 140 patients out of a total intake of 700. Eight
patients entering the Clinic presented moderately severe and severe Burn shock; 61 (43.6%)
developed the MOF syndrome. The control group of patients who did not develop MOF
consisted of 20 persons.
Table I presents the general characteristics of the burn trauma. The time preceding
commencement of care, as a constant value, does not appear to be of importance for the
outcome. For all patients, the time lapse varied between 30 and 35 min as patients were
transported only from the outskirts of the city of Sofia. In these patients the severity
of the burn was of substantial importance for the onset of the MOF syndrome.
Indices |
Group A
Healed /MOF |
Group B
Deceased/MOF |
Group C
CtrI without MOF |
Age (yr) |
41 ± 14 |
40 ± 13 |
35 ± 12 |
TBSA (%) |
33 ± 5 |
41 ± 9 |
35 ± 8 |
Full-thickness IIIB & IV
degree Burns |
9 ± 5 |
18 ± 10 |
8 ± 4 |
Facial burns (%) |
67 |
74 |
20 |
Upper airways burns and
toxic gas inhalation (%) |
27 |
39 |
- |
|
| Table 1 - Characteristics of thermal trauma |
|
Table II shows
the frequency of the different types of deficiencies in the course of the disease, and Table
III presents the complications due to nosological reasons. There was a very strong
correlative dependence (r > 0.91) between the complications of sepsis, pneumonia and
Curling's ulcer and the appearance of more than one function deficiency. Infectious and
inflammatory complications were thus a risk factor for the appearance.of the MOF syndrome.
The clinical manifestation of stress ulcers was a possible alternative to the development
of M017, and in this case the reason was acute anaemia and the appearance of hypoxaemia
combined with hypoxia.
Indices |
Group
A
n = 15 |
Group
B
B = 46 |
Group
C
n = 20 |
Cardiovascular
failure (%) |
100 |
100 |
100 |
Acute
respiratory failure |
27 |
78 |
- |
Acute renal
failure (%) |
20 |
63 |
- |
Acute
gastrointestinal failure |
27 |
37 |
- |
Hepatic failure
(%) |
53 |
87 |
- |
General
endocrine failure (%) |
33 |
89 |
- |
Immunological
failure (%) |
33 |
91 |
- |
Aplastic anaemia
(%) |
13 |
91 |
- |
|
| Table II - Frequency of acute internal
complications |
|
Indices |
r |
Group A
n = 15 |
Group B
n = 46 |
Group C
n = 20 |
Sepsis |
> 0.96 |
7
47% |
32
70% |
-
- |
Pneumonia |
> 0.94 |
4
27% |
22
48% |
-
- |
Curling's ulcers |
> 0.90 |
2
13% |
12
26% |
-
- |
|
| Table III - Frequency of main infectious
complications and Curling's ulcers |
|
The degree of deficiency, the rapidity and
order of appearance, and the response to medication were also important factors. In our
previous studies we established that in burns of up to 45% TBSA the endocrine system
reacts adequately by increasing hormone secretion. When burns exceed 45% TBSA, an
uncoordinated secretion of adaptive hormones continues until complete exhaustion.
The observation of immune reaction in cases of moderately severe and severe burns
indicates a tendency for low immune reactions around day 3 in the three groups (the
control group remained within the range of the reference values). In Group B this trend
persevered until the fatal outcome. In Group A patients the low immune reactions started
after day 3, attaining reference values around day 5-6. We have found in our studies that
the vigour of immunity and the possibility of its quick restoration depend not only on the
trauma severity but also on specific immunological features for each nation. The speedy
restoration of immunity is an excellent guarantee against infectious complications (Fig.
1). Our clinical material is here rather limited as this report is intended to be a
preliminary contribution.
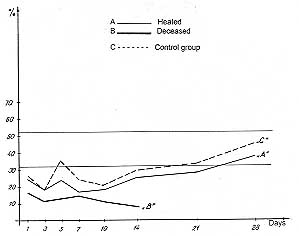 |
Fig. 1
- Immunity changes. |
|
Conclusion
The following groups of patients may be considered to be
exposed to the risk of N1OF syndrome:
- patients with severe burns (heavy shock)
- patients with complications of bacterial infections (sepsis
or pneumonia)
- patients with clinically manifested gastric or duodenal
stress ulcers
RESUME. Les Auteurs ont
effectué une étude prospective sur 700 patients brûlés traités à la Clinique des
Traumatismes Thermales de lInstitut N.1. Pirogov pendant une période de 34 mois. De ces
patients, 140 présentaient des brûlures modérément graves et graves. Le syndrome de
l'insuffisance organique multiple (IOM) a été trouvé dans 61 cas (43,57%). Les
critères pour diagnostiquer l'insuffisance d'un seul organe étaient les mêmes critères
de la nonne internationale. Si au moins deux fonctions organiques étaient critiquement
atteintes, les Auteurs ont exprimé une évaluation de 10M. Les patients atteints de IOM
ont été divisé en deux groupes: le groupe A (guéris - 15 patients) et le groupe B
(décédés - 46 patients). Un troisième groupe témoin (groupe C) contenait 20 patients
atteints de brûlures de gravité comparable, mais sans 10M, qui se sont tous rétablis.
L'analyse statistique a indiqué que les patients les plus exposés au risque de IOM
étaient: 1) les patients de sexe masculin âgés jusqu'à 50 ans et les patients de sexe
fémin âgés plus de 50 ans; 2) les patients atteints de brûlures des voies aériennes
supérieures, de brûlures dans plus de 30% de la surface corporelle, et de brûlures
profondes en plus de 10% de la surface corporelle; et 3) les patients qui ont présenté
la sepsis ou la pneumonie.
BIBLIOGRAPHY
- Baue A.: Multiple, progressive or sequential system
failure. Arch. Surg., 110: 779, 1975.
- Tilney N.I., Bailey G.I., Morgan A.P.: Sequential system
failure after rupture of abdominal aortic aneurysms. An unsolved problem in postoperative
care. Ann. Surg., 178: 117, 1973.
- Eiseman B., Beart R., Norton I.: Multiple organ failure.
Surg.Gynecol. Obst., 144: 323, 1977.
- Fry D.E., Pearlstern I., Fulton R.I., Polk H.C., Jr:
Multiple system organ failure. The role of uncontrolled infection. Arch. Surg., 115: 136,
1980.
- Fry D.E.: Multiple system organ failure. Mosby Year Book,
St Louis, 1992.
- Fry D.E.: Multiple organ failure. In: "Problems in
General Surgery", 10 (3), 564-78, J.B. Lippincott Co, Philadelphia, 1993.
- Saffle JR., Sullivan J.J., Tuohig G.M., Larson C.M.:
Multiple organ failure in patients with thermal injury. Crit. Care Med., 21: 1673-83,
1993.
- Polac H.C.: Factors influencing the risk of infection after
trauma. A Symposium: The continued challenge of trauma and infection in surgery. Amer. J.
Surg., 165 (2A): 2S-8S, 1993.
- Rodriguez J.L.: Hospital acquired gram-negative pneumonia
in critically ill, injured patients. A Symposium: The continued challenge of trauma and
infection in urgery. Amer. J. Surg., 163 (2A): 34S-42S, 1993.
- Baron P., Traber L.D., Nguyen T., Hollyoak M., Heggers
J.P., Herndon D.N.: Gut failure and translocation following Burn and sepsis. J. Surg.
Res., 57: 197-204, 1994.
- Moore F.A., Sauaia A., Moore E.E., Haenel J.B. et al.:
Postinjury multiple organ failure: a bimodal phenomenon. J. Trauma, 40: 501 -13, 1996.
- Henao F.J., Daes J.E., Dennis R.J.: Risk factors for
multiorgan failure: a case-control study. J. Trauma, 31: 74-80, 1991.
- Rixen D., Siegel J.H., Friedman H.P.:
"Sepsis/SIRS", Physiologic classification, severity stratification, relation to
cytokine elaboration and outcome prediction in posttrauma critical illness. J. Trauma, 41:
581-99, 1996.
- Simons R.R., Hoyt D.B., Winchell R.J. et al.: Elevated
selection levels after severe trauma: a marker for sepsis and organ failure and a
potential target for immunomodulatory therapy. J. Trauma, 41: 653-63, 1996.
- Darling G.E., Meresteci M.A., Ibanez D. et al.: Pulmonary
compaction in inhalation injuries with associated cutaneous Burn. J. Trauma, 40: 83-9,
1996.
- Petrov S., Ankov V., Yonov Y. et al.: Neurohormonal
metabolic and water-electrolytic disturbances in Burn shock and possibilities for their
correction. Final Report of the homonymous study. Military Medical Academy, Sofia,
Bulgaria, 1984.
- Vanev M., Ankov V., Yonov Y. et al.: Functional and dynamic
researches of adaptive systems in early phases of shock ("Dynamics"), Final
Report of the homonymous study, Military Medical Academy, Sofia, Bulgaria, 1987.
- Petrov S.: "Metabolic disturbances and multiple organ
failure in trauma, burns and infection", Military Publishing House, Sofia, 1984.
| This paper was received on 31 March
1998. Address correspondence to:
Dr Y. Yonov
N.I. Pirogov Emergency Institute
Sofia 1606, Bulgaria |
|