Annals of Burns and Fire Disasters - vol. XI - n. 3 - September 1998
ELECTRICAL BURN INJURIES
Babik J., Sandor, Sopko
Kosice Saca Burns Centre,
Slovakia
SUMMARY. The
distribution of burn injuries treated in the Saca Burns Centre in Kosice (Slovakia) is
documented. During the period considered (1971 -present day), electrical burns constituted
2.7% of all burn cases treated. With regard to the period between 1987 and 1994, a more
detailed study describes 96 patients treated for burns caused by electricity. The causes
of the burns and typology are described. The methods of treatment are also considered.
Introduction
Electrical injuries
represent a special type of thermal injury, with a pathophysiology depending on the
voltage, current flow and resistance of the skin. High-voltage electric current has
irreversible localized and systemic consequences, with a high percentage of disability.
Electrical injuries represent 2.7% of all burn admissions (12,930 patients since 1971) to
the Kosice Burn Centre. The pathological effects, the complications and the treatment are
discussed.
Since 1849, when commercial electricity became available, the potential danger of injury
has continued to increase.' According to statistical data, about 1% of accidental deaths
are caused by electric current. Electrical burns represent 2.7 % of all admissions to our
burns centre and the incidence is growing as the sources and use of electric power
continue to increase. Injuries due to contact with electricity most commonly involve
utility workers, and there is also a high incidence among children because of uncovered
electric lines. Household injuries from homemade equipment and repairs are very frequent.
The victims of electrical burns show certain specific features with regard to therapy and
the evolution of the pathology.
Electricity - as a flow of electrons - constitutes current, which depends on voltage and
amperage. The effect of the electric current on the body is determined by the following
seven factors: 1. type of current; 2. amount of current; 3. pathway of current; 4.
duration of contact; 5. area of contact; 6. resistance of the body; 7. voltage.
Flash or arc burns are usually superficial despite the fact that the arc generates
temperatures of over 10,000 °C.
Flash or are burns causing the ignition of clothing produce similar effects to those of
ordinary burns, with serious damage depending on the percentage of TBSA. Direct electrical
injury is due to the passage of current through skin, which is damaged either by the heat
generated or by a specific but as yet not well-defined effect on the body. It is generally
accepted that the severity of an injury is proportional to the intensity of current that
flows through the tissue.
Results
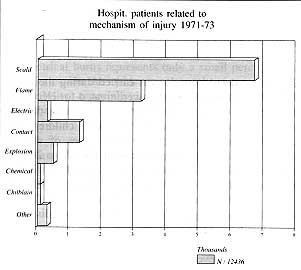
The distribution of burn
injuries in our Centre since 1971 is documented (Fig. 1).
|
Fig.
I - Distribution of burn injuries treated at the Kosice Saca Burns Centre, Slovakia
(1971-93). |
|
Electrical burn injuries
represented 2.7% of the total number of 12,355 admissions over this period, corresponding
to 347 patients. The total body surface area burned (TBSA) ranged from 1 to 91% (mean
area, 17.5%), but in electrical burns the mean TBSA was 5% and the range was from 1 to 8 1
%. Infection, one of the most important cause of complications, does not differ from that
found in non-electrical burns, with an incidence of 21.3% for Staphylococcus aureus and a
slight prevalence of gramnegative bacteria (Fig. 2).
|
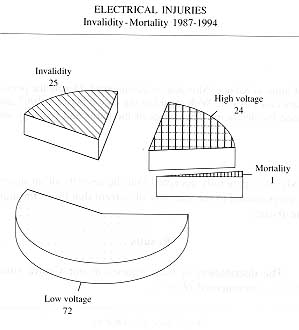
Fig.
2 - Disability and mortality. |
|
A more detailed study was
carried during the period 1987 - 1994. Ninety-six patients were treated for
electricityrelated burns. Of these, 24 (24.4%) were victims of highvoltage electric
current. Apart from three children, they were all linemen involved in various types of
working accidents. The voltage range was from 1000 V to 200 kV. One patient with
high-voltage injury (81% TBSA) died as a result of septic complications. All the patients
with highvoltage injuries sustained serious burns (TBSA 11-81%, mean 21%), with high
levels of morbidity and disability. Over a hundred operations were performed, including
nine amputations of the upper right arm and one shoulder disarticulation. Seven
amputations of the left arm were performed, with the seven forearms, and two
finger-andhand amputations. One patient with abdominal injuries underwent laparotomy with
reconstruction of a large defect of the peritoneum and abdominal wall. One complication of
high-voltage injuries was delayed healing due to impaired circulation, even in uninjured
parts of the extremities. In extensive electric burns the incidence of septic
complications was comparable with that of nonelectric burns. In the group of high-voltage
injuries, haemorrhage was accompanied by massive blood loss in 1% of cases.
One-quarter of fatalities due to electric power are caused by natural lightning energy. In
our area of the Tatry Mountains there is at least one case of this type of injury every
year. In the period of study, three patients were simultaneously injured by lightning. A
mother and her two children were struck by a bolt of lightning while sitting under an
umbrella in a mountain area. All three sustained Ill-degree burns to the head, buttocks
and feet, with 5% TBSA burns in one child and only puncture burns in the other two
victims. There was no effect of seizure or as regards breathing. The treatment was
complicated in one of the children, who presented slight epileptic activities documented
by EEG for six months post-injury.
Treatment
The treatment of electric
injuries has to be very careful because of the specific effect on nonviable tissue covered
by healthy uninjured skin. Considerable alterations occur in the microcirculation, with
the loss of endothelial integrity and the trapping of large volumes in the extravascular
space, leading to massive oedema and decreased circulation in the injured limb. Immediate
and adequate fluid resuscitation is therefore essential. The volume of resuscitation fluid
may be very large and unpredictable. In our study, the initial calculation of the fluid
was underestimated in every second patient. Every patient was carefully monitored in order
to avoid complications throughout treatment. Initial fluid management with Ringer's
lactate was administered in sufficient amounts to maintain a urine output of at least 50
ml/h. When myoglobinuria was present mannitol was administered.
Incision and fasciotomy were performed as soon as possible post-injury, with prompt
release of compression. Early necrectomy, extensive debridement and even amputation when
the injury was massive were necessary (Fig. 3). Fasciotomy and neural decompression
were necessary on the dorsal and volar aspects of the arm or lateral aspects of the leg.
Exposed nerves and tendons were covered with allografts until flap coverage was provided.
The hand and wrist were observed and decompression of the carpal tunnel was performed.
Full-thickness injury over major vessels should be debrided promptly and definitive
coverage provided as soon as possible. Small deep injuries have a slow spontaneous healing
and excision may be Of great help. Rotation or pedicle flaps and musculocutaneous flaps
were used. In some cases a free flap was the method of choice - this required a very
precise estimation of healthy vascular tissue. Coverage of the wounds by skin grafts was
delayed two or three days because of the high frequency of progressive necrosis of injured
tissue. We normally perform surgical excision on day 5 post-burn with reexcision and
coverage after 48 h. Extensive burns of the extremities and scalp pose a particularly
difficult problem in the acute phase as well as during reconstruction. For topical therapy
we used Sulfarnylon and silver nitrate.
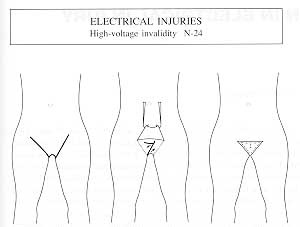
|
Fig. 3 - Amputation in 24 patients with high-voltage injuries. |
|
In cases of deep tissue
injuries, when for example tendons, bones and nerves are injured and necrotized, coverage
by some type of skin flap is the best treatment. Treatment utilizing pedicle skin flaps
usually gives good results but there may be major disadvantages such as discomfort and the
necessity of repeated operations. The free flap can resolve those problems. There is
however another problem in the use of the free flap - how to recognize which vessels in
the injured area are normal. Our experience with this type of surgery is very limited.
Discussion
Electrical burn injuries
represent a special type of lesion in which disability is high, and functional and
aesthetic sequelae very important.
The strategic management of high-voltage electrical injury can both challenging and
complex. The challenge begins at the moment of the injury and continues through the
rehabilitation period.
The complex aspects of management are the complications that occur owing to systemic
effects, mostly due to damaged arteries and veins, with the compression of oedema followed
by obliteration because of coagulation in the microcirculation, with a final effect that
may lead to amputation, usually of the upper extremities. In our series there was a
disability rate of 25% due to amputation of the upper extremities. Distribution by age and
sex was consistent with the findings of other researchers. Surgery was performed as soon
as possible in order to prevent lifeendangering complications, of which the most important
were infections and sepsis (46%), kidney failure (9%) and neurological complications (3%).
Cloud-to-ground lightning producing some hundreds of millions of volts, at a speed
exceeding a hundred thousand km per see, causes one-quarter of deaths from electrical
injuries.' Despite all preventive measures, we recorded every year one or more deaths and
a number of injuries of this type. Electrical burns represents only a small percentage of
burn injuries, but the incidence of complications, morbidity and disability, especially in
high-voltage injury, is high. All of those injuries are preventable.
RESUME. Les
Auteurs décrivent la distribution des brűlures traitées dans le centre des brűlés ŕ
Ko~icc (Slovachie). Pendant la période considérée (197 1 -aujourd'hui) les brűlures
électriques constituaient 2,7% de tous les cas de brűlures traités. Entre 1987 et 1994
une étude plus détaillée a considéré 96 patients traités pour des brűlures causées
par l'électricité. Les Auteurs décrivent les causes des brűlures, leur typologie et
les méthodes de traitement.
BIBLIOGRAPHY
- Artz C.P.: Changing concepts of
electrical injuries. Am. J. Surg., 128: 600, 1974.
- Jay K.M., Bartlett R.H. et al.:
Burns epidemiology. J. Trauma, 17: 943, 1977.
- Artz C.P., Moncrief J.A.:
"Burns - a Team Approach", p. 352. W.B. Saunders Co., Philadelphia, 1979.
- Hunt J.L. et al.: The
pathophysiology of electrical injuries. J. Trauma, 16: 335-40, 1976.
- Strasser E.J.: Lightning injuries.
J. Trauma, 17: 315-9, 1977.
This paper was
presented at the
Third International Conference held in Palermo, Italy
in June 1995.
Address correspondence to:
Dr Jahn BabiK
Kosice Saca Burns Centre
Slovakia. |
|