Annals of Burns and Fire Disasters - vol. XI - n. 3 - September 1998 ASPECTS OF RECONSTRUCTION IN ELECTRICAL INJURY Konigova R. Burns Centre, Third Medical Faculty, Charles University, Prague, Czech Republic SUMMARY. Between January 1984 and January 1998 an annual average number of 550 patients were admitted to the Prague Burn Centre, with an annual average of 700 in the last three years. Electrical injuries accounted for 4.6% of these cases. Apart from casualties with devastation of the upper extremities that necessitated amputation above or below the elbow, there were manifold other locations with extensive electrical injuries requiring an interdisciplinary approach in the Intensive Care Unit. Regarding reconstructive surgery, strictly individual decision-taking was indispensable. Decompressive surgery was accomplished immediately, simultaneously with resuscitation, followed by necrectomy every second day using xenografts as a temporary cover. For the permanent closure of exposed bones, tendons, joints or nerves various types of flaps were used. A special problem was encountered in cases with facial defects. The tubed flap technique, pioneered by our late Professor Francis Burian in 1912 and later recommended by Fitatov and Gillies, is still advantageous in some cases. This method can be performed under local anaesthesia using simple instruments at all stages. Patients with extensive burns and electrical injuries are severely compromised, and the use of free flaps (involving prolonged surgery under lengthy general anaesthesia) has to be a carefully taken decision. Introduction Electricity has been used to transmit power for only a century. As the demand for electricity increases, accident prevention techniques, as well as better methods for evaluation and treatment, must be developed. The longterm outcome of electrically injured patients is too often permanent disability. As most victims are young adults and children, the cost to victims, families and society is considerable. This presents a challenge to the medical community. An analysis of electric ity-related accidents causing burns was presented by Comini in 1992. Material and methods Despite all safeguards,
electrical injuries account for 4.6% of all admissions to the Prague Burn Centre. From
January 1984 to January 1998 we admitted an annual average number of 550 patients, with an
annual average of 700 patients in the last three years. Patients with highvoltage injuries
included boys aged 6 to 15 yr injured when playing on the roof of railway wagons or in the
neighbourhood of transformer stations, or when climbing electric pylons. Contact wounds
were found on the head and upper extremities.
A double-tube pedicle flap was raised to cover this defect, and simultaneously the vessels in the upper extremity were explored by the microsurgeon. To speed treatment up, the free muscular flap from the homolateral (left) m. latissimus dorsi was sutured into the defect (Fig. 3). Four days later thrombosis developed in the sutured veins and not only the flap but the whole hand was rendered cyanotic. The flap was removed and the hand was lost as well. The prepared tube might have been more successful in this case. The other contact on the boy's right foot was solved by means of another free flap taken from the other m. latissimus dorsi without any cornplications (Fig. 4).
Three months later, the stump of the left forearm was covered and modelled with the tubed flap; the patient is now ready for prosthesis (Fig. 5). The group of adults who sustained high-voltage injury at work included a 26-year-old electrician with deep contact burns in the chest and right forearm, and devastation of the left shoulder and elbow (Fig. 6). Two contact points were found on the head and back. The referring hospital did not report any unconsciousness, respiratory or cardiac arrest, or neurological abnormalities. Necrectomy was performed on day 3 after the accident and on day 14 the necrotic proximal part of the humerus and the lateral part of the clavicle were removed.
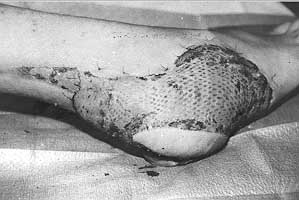
The stump of humerus was fixed to the scapula by means of cerclage. Ten days later the left shoulder was reconstructed by transposition of m. latissimus dorsi covered with meshed autografts overlaid with xenografts (Fig. 7). The defect in the temporoparietal region was solved with a rotation flap (local). At the same time the orthopaedic surgeon performed an osteosynthesis of the elbow joint by means of two Kirschner wires and the exposed bones were covered with a tube pedicle flap - prepared beforehand - in the left lower abdomen (Fig. 8). This recently married young man displayed severe emotional stress, but the birth of his child motivated his recovery.
Nine months later the patient was back at work, re-educated as a telephone operator in the same institute where he had previously been working as an electrician. The tube flap approached the destroyed shoulder for final modelling (Figs. 9a,b, 10).
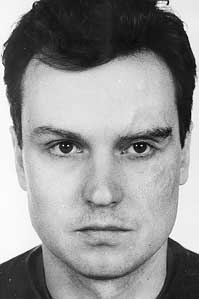
A special problem was encountered in cases with facial defects following low-voltage accidents. Two electricians who had suffered facial injuries from a 380 V electric shock were selected. A 29-year-old man with a contact burn in the supraorbital and zygomatic region was grafted and nine months later he asked for eyebrow reconstruction, having returned to work between times (Figs. 11, 12).
Another 21-year old man collapsed while working on an electrical panel, losing consciousness and suffering from cardiac arrest. Immediate cardiopulmonary resuscitation was initiated and on admission the patient was alert, although suffering from amnesia. The sensory and motor examinations were normal. X-ray of the skull and ECG showed no changes. The destruction of the temporal and periorbital region and the radix of the nose required necrectomies (Figs. 13a,b).
Xenografting was used to cover the defects temporarily, while a tube pedicle flap on the left arm was prepared (Figs. 14, 15a,b). Before transfer of one pedicle to the glabella region, the open frontal sinus was examined. All the flap surgery was carried out under local anaesthesia, without any antibiotics, because all the bacteriological swabs were repeatedly negative and there was no clinical sign of infection.
One year later the patient requested reconstruction of his post-traumatic saddle nose. An osteocartilaginous allograft removed from a cosmetic "hard" nose was used. The patient has since returned to work and married one of our patients (Figs. 16a,b, 17).
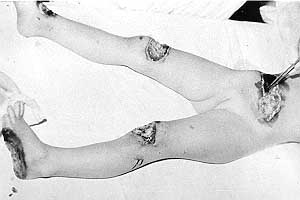
A unique case was that of a 4-year-old girl who fell from a fourth-floor window onto electric wires, which saved her life. She suffered deep necrosis of the trunk, both knees and the left foot. Early excision and suture on the trunk, full-thickness skin graft on the foot, and transposition flaps covering the open knee joints solved the situation (Figs. 18-20a,b). The patient has been followed up for 15 years without developing any sequelae.
Discussion Electrical injury, be it
low-voltage, high-voltage or superhigh-voltage in the form of lightning, may cause lesions
manifested as paraesthesia as well as carbonization or vaporization of a limb, complete
paralysis, and cardiopulmonary arrest! The basic change is electroporation of cell
membranes resulting in progressive necrosis superimposed upon a special type of burn. Any
organ may be involved. The uneven nature of the injury requires a multidisciplinary
approach in the intensive care unit. Conclusions For centuries, the
practice of medicine has been based on the assumption that physicians instinctively know
the right thing to do. We call this the "art of medicine", but procedures today
have become more complicated and not all of us can process all the acquired information
necessary to make the right decision for every patient. It has also been shown that
physicians have vastly different perceptions of the outcomes of different practices. This
is a result of the inappropriateness of different indications for various procedures. To
develop a guideline for the treatment of any disease it is necessary to retrieve all
evidence regarding the effectiveness of different treatments. Acknowledgements. The microsurgical procedures were performed by the team of Associate Professor Dr M. Tvrdek, Head of the Department of Plastic Surgery, Third Medical Faculty, Charles University, Prague.
RESUME. Dans la période janvier 1984-janvier 1998 le numéro moyen annuel de patients hospitalisés dans le Centre des Brűlés de Prague était 550 (700 dans les derniers trois ans). Les lésions électriques constituaient 4,6% de ces cas. A part les patients qui ont subi la dévastation des extrémités supérieures qui ont nécessité l'amputation au-dessus et au au-dessous du coude, nous avons observé d'autres sites avec des lesions électriques étendues qui ont nécessité une approche interdisciplinaire dans le Service de Réanimation. Pour ce qui concerne la chirurgie reconstructive, il fallait absolument prendre des décisions selon les cas individuels. La chirurgie décompressive a été effectuée immédiatement, en męme temps que la réanimation, suivie par la nécrectomie tous les deux jours, avec l'emploi de xénogreffes comme couverture provisoire. Pour couvrir en maničre permanente les os, les tendons, les articulations et les nerfs exposés nous avons employé divers types de lambeau. Les défauts du visage ont présenté un problčme particulier. La technique du lambeau tubulaire, inventée par notre regretté professeur Francis Burian en 1912 et perfectionnée par Filatov et Gillies, présente toujours certains avantages. Cette méthode peut ętre réalisée avec une anesthésie locale, utilisant des instruments trčs simples pendant toutes les phases. Les patients atteints de brűlures étendues et de lésions électriques sont sévčrement compromis, et l'emploi des lambeaux libres (qui nécessitent de longues procédures chirurgicales en anesthésie générale) doit ętre toujour une décision attentivement pesée. BIBLIOGRAPHY
|