Annals
of Burns and Fire Disasters - vol. Xl - n. 3 - September 1998
TEMPORARY WOUND DRESSING OF BURNS
WITH FRESH, STERILE, FROZEN PORCINE SKIN
Becker D.
Department of Emergency,
Academic Training Hospital, Bad Hersfeld, Germany
SUMMARY. In
1964 Kohnlein described seven severely burned patients who received a primary wound
dressing of fresh porcine skin, with reasonable success. When fresh, frozen, sterile
porcine skin became readily available as a dressing, our hospital in Bad Hersfeld
(Germany) adopted this primary wound dressing as a regular part of its planning of burns
treatment. Today, the use of cadaver skin as a better biological dressing has been
discontinued because of the danger of HIV infection, and the expectations raised by the
culture of epithelial cells have not been fully realized: the culturing is very expensive
and the sheets transplanted become necrotic in most patients after six months. It is thus
necessary to revive the use of porcine skin wound dressing. Porcine skin is available as a
collagenate (Mediskin), which can be stored without any problems. And pigs are to be found
all over the world
Introduction
A burn accident is a most
spectacular occurrence, and often the most conspicuous consequence is extensive injury to
the integument. The early covering of burn wounds with grafts decisively influences the
further clinical course - as well as shock therapy and rapid parenteral fluid supply,
according to well-known calculable parameters.
In 1964, for the first time in Europe, Kohnlein produced a report on the
heterotransplantation of porcine skin as a therapeutic measure in burn patients. In Kings
County Hospital, New York, seven severely burned persons with over 50% body surface burns
were successfully treated using primary wound dressings of fresh porcine skin.
The autograft coverage of burn wounds is virtually impossible because of the additional
suffering caused to the patients. A combination of auto- and allograft skin
transplantation requires a large number of blood donors, who are hard to find in such
numbers.
The white skin of pigs seems to be an adequate substitute for skin homografts, for the
following reasons:
it has a surprisingly
similar structure to that of human skin
it has an extremely low
content of proteolytic enzymes, which accounts for its great resistance capacity
there is no connection
between the graft and the vascular system of the recipient. Consequently this cannot
become the object of an antigenic antibody reaction. Also for this reason there cannot be
any local or general toxic reaction
there is a distinctive
epithelialization effect
Method
On the basis of the above
considerations, we have applied early wound coverage in burn victims at the Surgery
Department of the Hospital in Bad Hersfeld since 1969.
The first very severely burned patients were seven children with first-, second- and
third-degree burns in 6070% body surface area. They were treated with fresh porcine skin
and they all survived. This positive result was the reason for our decision to include
this measure among our therapeutic protocols as an indispensable lifesaving method.
Necrotic tissue has to be removed after the shock phase has subsided, within the first 48
h, when burns are sterile because of the effect of heat. In the course of the same
operation the entire area of the burn wound has to be covered with porcine skin (Fig. 1).
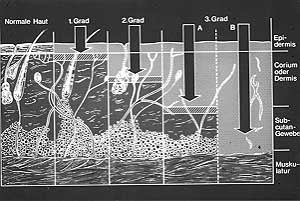 |
Fig.
1 - Different areas of cutis damaged by heat. These specific areas determine the
graduation of the burn status. |
|
Back in 1969 it was rather
difficult to obtain fresh porcine skin. In case of need, a team had to be sent to the
local slaughterhouse and skin was removed, under sterile conditions, from freshly
slaughtered pigs. After repeated washing with penicillin solution, the porcine skin was
ready to be placed on the wound. The skin bonded tightly to the wound after only a few
minutes, and it was possible to continue with "open wound" treatment (Fig.
2). This complicated manner of obtaining fresh porcine skin has now been considerably
facilitated. Fresh sterile porcine skin is now available as Mediskin in a frozen state. It
is sealed in plastic packages and can be supplied in the required quantity.
 |
Fig.
2 - Child's face, first- and second-degree burns. Burned areas covered with fresh
sterile frozen porcine skin. The immediate adherence of the protein-rich fluid of the
wound is visible. We thus have open wound treatment conditions. |
|
After despatch by express
mail it can be stored for up to 18 months a normal freezer without any problems. Thus, in
the event of an emergency, a sufficient supply of porcine skin can always be guaranteed.
When required, Ringer's or normal saline solution is placed directly into a vessel. After
two minutes the porcine skin thaws and is ready for use. The prepared gauze is positioned
directly opposite the wound surface and, after adjustment of the graft to establish the
contour of the wound, the porcine skin is placed in position without any difficulty.
Subsequent treatment of the wound is similar to that used in open wound treatment.
Results
We have used this kind of
early wound coverage in burn victims for nearly 20 years, treating 296 burn victims. The
youngest patient, two years old, had extensive first-, second- and third-degree burns in
the right hand, arm and thorax due to scalding. The oldest was 72 years old. All the burns
treated with Mediskin presented ideal conditions, without severe infection, and good
epithelialization effect.
The survival of severely burned middle-aged persons is always difficult, but using this
therapy good results can be obtained. When porcine skin has been placed on the wound, it
quickly adheres because of the extremely high protein content of the exudate. Nearly total
wound closure is thus achieved. The otherwise enormous loss of fluids, electrolytes and
proteins can considerably be reduced and more easily controlled. Equally important is the
prevention or at least the reduction of the risk of infection in extensive wound areas,
which are a perfect base for contamination and a breeding site for infective agents of all
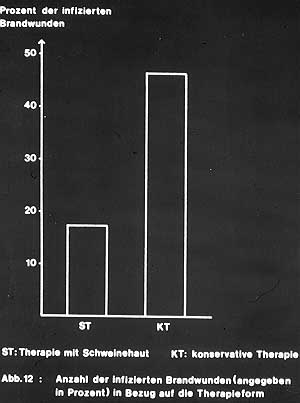
kinds. The parenteral supply of antibiotics alone cannot achieve effective levels in the
burn area (Fig. 3).
|
Fig.
3 - Low rate of local infection achieved with use of primary wound dressing with fresh
sterile frozen porcine skin. |
|
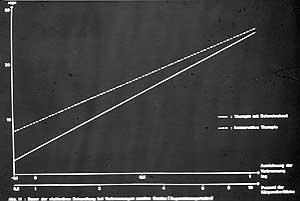
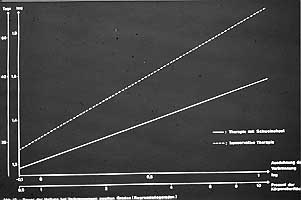
The healing process of
burns is accelerated by the use of porcine skin. Comparison with a group of patients
receiving the previously used standard local treatment showed a significant reduction in
hospital stay and in healing time (Figs. 4, 5). A further advantage of the Mediskin
temporary wound dressing is the inexplicable but immediate relief from pain that is much
welcomed by the grateful patients. We can therefore significantly reduce the amount of
analgesics that have to be used.
|
|
Fig. 4 - Reduced post-burn hospitalization following use of
Mediskin wound dressing. |
Fig. 5 - Duration of local wound healing significantly
reduced compared with that of control group treated with traditional methods. |
|
Discussion
The advantages of early wound dressing are
evident. In addition to its immediate adherence to the wound bed, the use of Mediskin
leads to:
- a significant reduction in the loss of
proteins, electrolytes and fluids. There is also a significant reduction in the amount of
infusions on the basis of laboratory parameters
- a reduction in the risk of infection, due
to the considerably smaller contamination area
- the possibility of using open wound
treatment conditions, as further wound dressings become unnecessary. After
epithelialization of the wound, the porcine skin dries and either comes away by itself or
can be peeled off, when another piece of porcine skin can be positioned in the same
manner. Permanent changes of wound dressings become redundant
A considerable relief of
pain immediately occurs that allows a reduction in the use of analgesic drugs, and early
mobilization - particularly with gymnastic exercises - can be initiated. We have thus been
able to treat successfully a number of severely burned hands and restore satisfactory
functioning (Figs. 6-8).
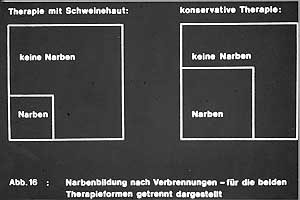
Slight cicatrization effects after the healing process have thus been overcome.
Particularly disfiguring keloid formations have not been subject to research in our
hospital.
Summing up all our experience in the field of primary wound dressing using fresh sterile
frozen porcine skins on burns, we can say that our results show the very best local
therapy for burned patients at the present time.
 |
Fig.
6 - Local situation of severely burned hand. |
|
 |
 |
Figs. 7a/b - Satisfactory function of burned hand obtained
by wound dressing with fresh sterile frozen porcine skin. |
|
 |
 |
Fig.
8 - Right-hand side indicates relationship between "slight cicatrization effecC
and keloid formations. |
Fig.
9 - Face of boy shown in Fig. 2 treated using primary wound dressing consisting of
fresh sterile frozen porcine skin (Mediskin). |
|
Conclusion
Today, the use of porcine
skin is limited. This is because the skin of cadavers is widely preferred in view of its
more biological effect and also because of recent medical expectations with regard to
epithelial cultured skin support. However, cultured skin substitutes are very expensive -
a sheet measuring 10 x 10 cm costs some thousands of Deutschmark - and after about
six months the supports themselves also become necrotic. Also, cadaver skin is no longer
available due to Hiv infections.
Some publications have recommended shark skin as an ideal first-time wound dressing. But
this means neglecting the advances of Mediskin - a collagenoid of porcine skin - and the
excellent results achieved and documented in past decades. And why should an endangered
species like the shark be sacrificed when another animal is so widely available?
RESUME. En
1964 K�hnlein a d�crit le traitement de sept patients gr�vernent br�l�s qui ont re�u
un pansement primaire pour leurs l�sions constitu� de peau fra�che porcine. Les
r�sultats ont �t� positifs. Quand la peau porcine fra�che et congel�e commen�ait �
�tre facilement disponible comme pansement, notre h�pital � Bad Hersfeld a adopt� ce
pansement primaire des l�sions comme une proc�dure normale dans le traitement routinier
des patients br�l�s. Aujourd'hui l'emploi de la peau de cadavre comme pansement
biologique pr�fer� a �t� abandonn� a cause du danger de l'infection HIV, et l'espoir
une fois suscit� par la culture des cellules �pitheliales n'a pas �t� totalement
realis�: la culture est tr�s co�teuse et les lambeaux transplant�s se n�crotisent
dans la plupart des patients apr�s six mois. Il faut donc r�examiner la possibilit�
d'employer le pansement de peau porcine. La peau porcine est disponible comme collag�nate
(Mediskin), qui peut �tre conserv� sans difficult�. Et les cochons se trouvent en tout
le monde!
BIBLIOGRAPHY
- Masellis M., D'Arpa N., Napoli
B.: Considerations on intensive care in elderly burn patients. Anti. Burns and Fire
Disasters, 7: 207-13,1995.
- Kohmlein. In: Stengel W.: Die
Behandlung von Verbrennungswunden. Heft UDfallheilkunde, 94: 295-8, 1967.
- Stengel W.: Die Behandlung von
Verbrennungswunden Unfallheilkunde, 94: 295-8, 1967.
- Aronoff M., Flieschmann P., Simon
D.L.: Experience in the application of porcine xenografts to split-graft donor sites. J.
Trauma, 16: 280, 1976.
- Stinson V.: Porcine skin dressing
for burns. Am. J. Nurs., 74: 111 - 2, 1974.
- Toranto I.R., Styler K.E., Myers
M.B.: Vascularisation of porcine skin heterografts. Plast. Reconstr. Surg., 54: 195-200,
1974.
- Seeker D.: Erfahrungen mit
passagerer Deckung von Verbrennungswunden mit frischer-steriler-gefrorener Schweinehaut.
Unfallheitkunde, 84: 158-60, 1991.
- Becker D.: Erfahrungen mit
passagerer Deckung von Verbrennungswunden mit frischer, steriler, gefrorener Schweinehaut.
Der Krankenhausarzt, 56: 982-7, 1998.
- Krupp S.: Zur Deckung von
Verbrennungen und Korrektur Verbrennungsnarben mit Spalthautmaschentrasplant.
Unfallheilkunde, 81: 28-30, 1979.
- Becker D.: Tempor�re Wunddeckung
mit frischer, steriler, gefrorener Schweinehaut. Der Krankenhausarzt, 56: 982-7, 1983.
- Becker D.: Mit Schweinehaut den
Defekt gedeckt. Selecta, 16: 938, 1989.
This paper was
received on 9 March 1998.
Address correspondence to:
Dietrich Becker M.D.
Accident Surgery Department of the Academic Training Hospital
Seilerweg 29, 36251 Bad Hersfeld, West Germany. |
INFORMATIC
UPDATE
Informatic
Update is a new feature that we shall be publishing regularly as from the next issue
of Annals. Our aim is to create a space where we can inform our readers about new
developments in information technology and review any new products which they may wish to
submit to our attention.
Information science has taken on an ever more important role in the medical field in the
last few years and the computer is now an irreplaceable work tool, especially for data
storing and processing. However, our years of experience with computerization at the
Department of Plastic Surgery and Burns Therapy in Palermo have led us to believe that the
computer can also be applied more specifically in the clinical field.
At present not many such clinical application exist, mainly because medical software can
only be developed by persons who are competent in the two fields of medical and
information science.
Another purpose of this new feature is to stimulate collaboration among all those who -
like us - believe in the future development of the clinical application of the computer
and to attract the attention of people who are not yet fully aware of the computer's
potential. Relevant articles and actual applications can be sent to the address below:
Annals of
Mediterranean Club for Burns and Fire Disasters (MBC)
Informatic News
Divisione di Chirurgia Plastica e Terapia delle Ustioni.
Ospedale Civico, Via Carmelo Lazzaro, 90127 Palermo, Italy
E-Mail: mbcpa@cres.it
MBC - PREVENTION
CAMPAIGN
The MBC, in the context of the activities laid down in its Statute and
intended to promote burn prevention campaigns, has produced the following videotapes:
The Prevention of
Burns in Children
The Prevention of Electrical Burns in Everyday Life
The Prevention of Electrical Burns at Work
The Prevention of Industrial Disasters
How to Defend ourselves from Fire
How to Defend ourselves from Forest Fire
The tapes have been
dubbed in English, French, Arabic, Italian, Spanish, Greek and Turkish and come in two
versions, U-MATIC and VHS.
All the tapes are available entirely free of charge to MBC Members who apply in writing to
receive them explaining their reasons and undertaking to use them exclusively to promote a
burn prevention campaign in their respective countries.
For non-members of MBC the tapes are available at a cost of US$ 25 each, including postal
charge.
Please address
requests to: Annals of Burns and Fire Disasters, Divisione di Chirurgia Plastica e Terapia
delle Ustioni, Ospedale Civico, Via C. Lazzaro, 90127 Palermo, Italy, Tel.: + 39 916663631
- Fax: + 39 91 596404. |
|