| Annals of Burns and Fire Disasters - vol. XI - n. 4 - December 1998
BURN INJURIES IN
BENGHAZI: EIGHT YEARS STUDY
El-Gallal A.R.S., Yousef S.M., Toweir A.A.
Burn Unit, Aljala Hospital, Benghazi, Libya
SUMMARY. This study evaluates
thermal injuries in the region of Benghazi, Libya. From January 1990 to December 1997,
6797 patients were treated in the Burn Unit at A1jala Hospital, Benghazi. The frequency of
burns increased every year, being more frequent in the cold season. All serious burned
patients from hospitals outside Benghazi (25.7%) were referred to our unit. Young adults
(48.9%) were the most commonly involved, followed by infants and children (35.9%), while
elderly patients with burns were infrequent (1.5%). Overall, scald accidents were the
commonest cause of thermal injuries (47.2%), followed by flame burns (34.9%). Scalding was
the also the main cause of burns in infants and children, while among adults burns were
mostly caused by flame. The male to female ratio was 1: 1. 1. Home accidents accounted for
68.3 % of our patients, of whom 69.8 % were females. Work accidents were responsible for
only 21.2% of the injuries. Suicide attempts were generally infrequent (0.6%) but were
relatively more frequent among females. The mean BSA was 23.8% (12.7%) and the overall
mortality was 19%. Non-Libyan patients (mostly adult males) accounted for 9.6% of the
cases. Diabetes was the commonest associated medical condition found in our patients
(10.7%). The data obtained in our study are discussed and compared those of similar
studies carried out elsewhere.
Introduction
As in many fast-developing countries,
burn epidemiology in Libya is still at an early stage of development and few studies are
available to date. The aim of this hospital-record based study was to make a recent
estimate of thermal injuries in the region of Benghazi and surrounding towns. Our study
was carried out at the main referral hospital in the region.
Our burn unit is based in A1jala Hospital, Benghazi, which serves the city as well as the
eastern part of the country (population over two million). The unit consists of 40 beds
for paediatric and adult females, and 12 separate beds for adult males. Severely burned
patients are accommodated initially in the intensive care unit.
Methods
This study started in January 1990 and
ended in December 1997. All the required data were recorded on special cyclostyled forms.
The data included the age, sex, residence and nationality of the patients, causes, date
and extent of the burn, place, type and nature of the injury, and concomitant medical
condition.
For the purposes of the study the patients were grouped according to age into five groups
(less than 5 yr, 6-12 yr, 13-40 yr, 41-65 yr, and more than 65 yr). The patients were also
grouped according to their burned surface area (% BSA) in 10 categories, ranging from I to
100%. The nature of the injury was defined in this study as either accidental or suicidal.
As per the existing policy of our unit, the Evans formula was used for fluid replacement.
Locally, povidone-iodine (Betadine) was used as a standard treatment, as also silver
sulphadiazine cream (Flamazinel). Autografting was the only skin grafting procedure used
in our unit.
Results
Over a period of eight years, 6797
patients presented to our Unit. The annual frequencies of our patients during the years
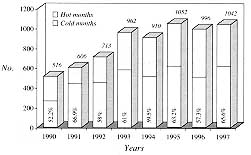
under review are shown as a histogram in Fig. 1.
 |
 |
| Fig. 1
- Annual and seasonal frequencies. |
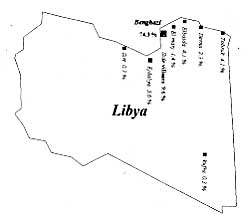
Fig. 2 -
Geographical distribution of patients. |
|
The histogram shows that more than 50% of
the annual number of accidents occurred in the cold season (OctoberMarch).
Of our patients, 25.7% (1744 / 6797) were referred from various peripheral hospitals
outside the city of Benghazi (Fig. 2). These patients were mostly seriously
injured.
Table I shows age distribution and the causes of the burns, also in relation to the
age group. Patients aged between 13 and 40 yr constituted 48.9% of the total number (3324
/ 6797), while patients under 13 yr accounted for 35.9% (2440 / 6797).
Admission of patients over the age of 65 years was infrequent, representing only 1.5% (102
/ Table 1 - Relationship between cause of burn and age of patients 6797). The youngest
patient was a new-born male two days old, while the eldest was a female of 83 years. The
mean SD) age was 24 yr (± 18.4).
Overall, scald accidents accounted for 47.2% of thermal injuries (3208 / 6797), with
15.6%, 12.4%, 10.6% and 8.6% of scalds being caused respectively by boiling water, hot
food or oil, tea or coffee, and hot milk. Flame burns were found to be the second
commonest cause of injury, accounting for 34.9% of cases (2371 / 6797). Of these flame
burns, 13.8%, 11.2% and 9.9% were caused respectively clothes by catching fire,
cooking-gas explosions, and direct exposure to flame. Scalding accounted for 84.9% of
thermal injuries (1091 / 1285) in preschool children, and of these injuries 55.1% (636 /
1155) involved children aged between 6 and 12 yr. Flame burns predominated over other
causes of burns that affected both adults and the elderly age groups, being responsible
for 44.2% and 40.2% of their thermal injuries respectively (1880 / 4255 and 41 / 102).
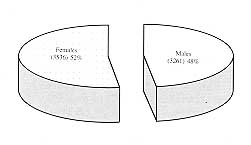
Although 51% of the patients aged 13-65 yr were males (2222 / 4357), females (3536 / 6797)
overall outnumbered males (3261 / 6797) (male to female ratio, I / 1. 1 (Fig. 3).
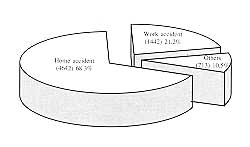
Among our patients 68.3% (4642 / 6797) sustained their injuries at home, and of these
patients 69.8% were females (3240 / 4642). Overall, 31.7% of the total number (2155 /
6797), mostly adult males, suffered their accidents outside the home, of which 21.2% (1442
/ 2155) occurred at the place of work (Fig. 4).
The nature of the injury was accidental in 99.4% of the patients (6756 / 6797). Suicide
attempts accounted for only 0.6% of the case (25 females and 16 males), of whom nineteen
(7 females and 12 males) were known to be undergoing psychiatric treatment (Table II).
Causes of burn |
Age groups (yr). |
0 - 5 |
6 - 12 |
|
> 65 |
All age groups |
Scald |
1091 84.9%
34.0% |
636 55.1%
19.8% |
1450 34.1%
45.2% |
31 30.4%
1.0% |
320 8 47.2%
100% |
Flame |
65 5.1%
34.0% |
385 33.3%
19.8% |
1880 44.2%
45.2% |
41 40.2%
1.0% |
2371 34.9%
100% |
Electrical |
81 6.3%
15.4% |
64 5.5%
12.2% |
379 8.9%
72.2% |
1 1.0%
0.2% |
525 7.7%
100% |
Contact |
48 3.7%
10.0% |
67 5.8%
13.9% |
338 7.9%
70.0% |
29 28.4%
6.0% |
482 7.1%
100% |
Chemical |
0 0.0%
0.0% |
3 0.3%
1.4% |
208 4.9%
98.6% |
0 0.0%
0% |
211 3.1%
100% |
All causes |
1285 100%
18.9% |
1155 100%
17% |
4255 100%
62.6% |
102 100%
1.5% |
6797 100%
100% |
| |
2440
35.9% |
|
|
|
5764
84.8% |
|
Table I - Relationship
between cause of burn and age of patients |
|
 |
 |
| Fig. 3 -
Distribution of patients by sex. |
Fig. 4 -
Distribution of patients by place of accident. |
|
The mean BSA (±) SD in our patients was
23.8% 12.7%) (range, 1-100%). There were no deaths among patients who sustained burns of
less than 7% BSA, while there was a 100% death rate in patients,with a BSA exceedino, 70%.
There were no survivals among infants and children under the age of 4 years and the
elderly over 65 years who had a BSA of more than 50% (Table III). The overall
mortality rate was 19% (1290 / 6797), and among the deceased patients 81% (1045 / 1229)
died between 12 and 24 days post-burn.
| Nature of burn |
Number
of patients |
Percentage |
| |
Male |
Female |
| Accidental |
6756 |
3245 |
3511 |
99.4 |
| Suicidal |
41 |
16 |
25 |
0.6 |
Psychiatric |
19 |
12 |
7 |
|
|
| Table II - Distribution by nature of burn injury |
|
Age
groups
(yr) |
Age
groups (yr) |
1 -
10% |
11 -
20% |
21 -
30% |
31 -
40% |
41 -
50% |
51 -
60% |
61 -
70% |
71 -
80% |
81 -
90% |
91 -
100% |
0 - 5 |
496 |
355 |
224 |
127 |
43 |
23 |
9 |
6 |
3 |
0 |
6 - 12 |
384 |
349 |
217 |
107 |
45 |
28 |
15 |
8 |
2 |
0 |
13 - 40 |
697 |
712 |
529 |
409 |
394 |
324 |
179 |
64 |
8 |
8 |
41 - 65 |
189 |
258 |
189 |
111 |
89 |
41 |
31 |
14 |
6 |
3 |
> 65 |
24 |
27 |
17 |
13 |
11 |
6 |
3 |
1 |
0 |
0 |
All age
groups
% |
1790
26.3% |
1701
25% |
1175
17.3% |
767
11.3% |
582
8.5% |
422
6.2% |
237
3.5% |
93
1.4% |
19
0.3% |
11
0.2% |
Deaths |
73* |
202 |
314 |
183 |
102 |
117 |
176 |
93 |
19 |
11 |
All
sustained more than 7% and mainly babies and senile patients. |
|
| Table III - Relationship between age, BSA and mortality |
|
Among our patients 9.6% (652 / 6797) were
nonLibyans, the majority being adult: males (Table IV).
The concomitant medical conditions reported during the years under review are shown in Table
V.
Nationality |
Number
of patients |
Percentage |
Libyan |
6145 |
90.4 |
Non-Libyan |
652 |
9.6 |
|
201 |
|
|
120 |
|
|
115 |
|
|
103 |
|
|
113 |
|
|
Table IV
- Nationality of patients |
|
Medical condition |
Number of patients |
| |
Male |
Female |
Frequency |
| Diabetes mellitus |
727 |
195 |
532 |
10.7% |
| Respiratory illness |
136 |
41 |
95 |
2.0% |
| Muscular disorders |
102 |
84 |
18 |
1.5% |
| Cardiac diseases |
82 |
36 |
46 |
1.2% |
| Psychological disorders |
54 |
31 |
23 |
0.8% |
| Epilepsy |
27 |
6 |
21 |
0.4% |
| Mental retardation |
20 |
4 |
16 |
0.3% |
| Hepatitis |
20 |
12 |
8 |
0.3% |
| HIV infection |
3 |
2 |
1 |
0.04% |
|
Table V
- Concomitant medical conditions |
|
Discussion
The pattern and frequency of burns in
various parts of the world seem to have wide variations. Also, the lack of uniformity
between methodologies, in addition to the existence of a plethora of variables and
differences in the periods of study, makes any comparison with other studies difficult.
The annual rate of thermal injuries in our area has increased gradually every year. This
could be attributed to an increasing incidence of scalds among children and adult females
and to an increase of flame burns among adult males.
The seasonal peak that has been observed in the cold months of the year could be explained
by the occurrence of accidental burns related partly to the improper use of gas and
kerosene for heating purposes and partly to the widespread custom of preparing hot drinks
in the sittingroom. Of our patients 84.8% (5764 / 6797) were aged less than 41 yr, with
48.9% and 35.9% of the total number occurring in adults aged 13-40 yr and children below
13 yr, respectively. This means that the order of frequency of thermal injuries affecting
different age groups is not consistent with that reported by other researchers.` This
could be attributed to the high proportion of young adult females who sustained burns at
home. In addition, most of our patients burned outside the home were young adults.
The infrequency of elderly burned patients in our society (1.5%) is similar to that
observed in Kuwait,' but contrasts with that found in England and Wales' and France,`
where patients over 60 and 65 yr presented a high frequency respectively of 11% and 13%.
This disparity could be explained by differences in population structure and by the fact
that most of our elderly population are sedentary and cared for by other family members,
and thus kept away from potential hazards.
Scalding was the leading cause of thermal injury in our society, being responsible for
47.2% (3208 / 6797) of the total number of injuries. Of these, 53.8% (1727 / 3208)
occurred in children under the age of 13 yr. The frequencies of scalding in each of the
age groups (84.9%, 55.1%, 34. 1 % and 30.4%) were higher than the figures found in
comparable age groups elsewhere (64%, 34%, 17% and 21 %).
With regard to flame-burned patients, in the different age groups, the opposite was true,
since our cases presented a low frequency (5.1%, 33.3%, 44.2% and 40.2%) as compared with
that observed in comparable age groups (18%, 58%, 58% and 72%) in the abovementioned
study.
A female predominance was encountered in our study, consistently with reports from
Algeria" and Kashmir.` This is however in contrast with results from other areas like
Jordan,`Japart, 14 Australia` and Virginia.` To a large extent, we can attribute this
finding to a high female presence among in our domestic burn patients (69.8% = 3240 4642).
Nevertheless, the frequency of domestic injuries (68.3%) was', relatively low as compared
with other studies, in which it ranged between 71 and ~0%.
Only 41 patients (0.6%) were managed as attempted suicide cases~and, of these, nineteen
were known to be under psychiatric care. Although statistically insignificant, it is
interesting to note that the male/female ratio among patients without any psychiatric
disorders was 4/18.
It was found that the BSA of most infants and children ranged between 1 and 10%, while
that of most adults ranged between 11 and 20%. This could be attributed to differences in
the main causes of burn, since scalds in children, which were frequently caused by hot
drinks, usually affected relatively limited surface areas compared with those caused by
flame burns in adults and the elderly. Also, our mean percentage BSA (23.8 ± 12.7%) is
relatively high compared with the 15% found by French authors. This could be explained by
the presence in our patient population of a significant proportion of referred cases
(25.7%) with an extensive BSA.
The overall mortality was 19% (1290 / 6797). Although this was higher than the mortality
rates ranging from 7.2 to 9.5% reported'by others, we consider that our finding is
proportional to the relatively high number of patients who were referred to our unit
either in late stages of their illness or with serious injuries. Eighty-one per cent of
deaths were attributed mainly to burn wound sepsis and its consequences. The contributing
factors in the remaining 19% were inhalation injuries, acute renal failure, cardiac
arrest, and the presence of concomitant serious illness.
The non-Libyans who accounted for 9.6% of our cases were mostly labourers and technicians
from various countries. Many nationalities were involved in this group of patients but
expatriates from Egypt, Sudan, Palestine and Chad were those most commonly afflicted. This
could be attributed to their relatively high presence in our community. As said, they were
mostly manual labourers, and their living standards were far below average, with work
safety precautions that were far from ideal.
It is noteworthy that diabetes was observed in 10.7% of our patients, which contributed
considerably to morbidity levels, while other medical conditions were less common. The
frequency of psychiatric disorders (0.8%) in our study was not comparable with the 7%
reported by French authors.
On the other hand, the number of our epileptic patients (27) was certainly high, in spite
of their low representation (0.4%), as compared with the 14 epileptic patients Address
correspondence to: Dr A.R.S. EI-Gallal, Burn Unit, Aljala Hospital, Benghazi, Libya.
reported by others` over a much longer period of 16 years. Although it is desirable to
perform epidemiological studies in developing countries like ours on a nation-wide basis,
we believe that the data we present here provide a fair idea of the pattern of thermal
injuries that occur in this region of our country.
RESUME. Les Auteurs se
proposent d'évaluer les brûlures dans la région de Benghazi (Libye). Pendant la
période janvier 1990décembre 1997 6797 patients ont été traités à l'Unité des
Brûlures de l'Hôpital Aljala, Benghazi. La fréquence des brûlures a augmenté tous les
ans, avec une fréquence majeure dans la saison froide. Tous les brûlés graves non
résidents à Benghazi atteints de graves brûlures (25,7%) ont été hospitalisés dans
notre Unité. En général, les patients les plus fréquemment atteints étaient les
jeunes adultes (48,9%), suivis par les enfants (35,9%). Les patients âgés étaient
rarement atteints (1,5%). La cause la plus fréquente des brûlures était
l'ébouillantement (47,2%), suivie par la flamme (34,9%). Chez les enfants
Fébouillantement était la cause principale, et chez les adultes elle était la flamme.
Le rapport mâle/femelle était 1 : 1,1. Les accidents domestiques constituaient 68,3% des
cas, dont 69,8% fémelles. Les accidents professionnels constituaient seulement 21,2% du
numéro total. Les tentatives de suicide étaient rares (0,6%). La surface moyenne
brûlée était 23,8% (+12,7%) et la mortalité complessive 19%. Les patients non libyens,
pour la plupart des patients adultes mâles, constituaient 9,6% du numéro total. La
pathologie la plus fréquente était le diabète (10.7%). Les Auteurs en conclusion
discutent leurs résultats et les comparent avec des études similaires effectuées
ailleurs.
BIBLIOGRAPHY
- Akhtar M., Gang R.K.: Epidemiology of burns in Benghazi,
Libya. Burns, 7: 351, 1981.
- Zaidi M.M., Abussetta A. et al.: Analysis of burned
children treated in the burns and plastic surgery centre, Tripoli, Libya, in the year
1992. Ann. Medit. Burns Club, 6: 217-23, 1993.
- Zaidi M.M., Abussetta A. et al.: Management of severely
burned patients - a study of 684 severely burned patients admitted in the last six years
to the burn and plastic surgery centre, Tripoli, Libya. Ann. Burns and Fire Disasters, 9:
3-7, 1996.
- Belba G.J., Andrea A. et al.: Some epidemiological data
regarding burn patients treated during 1992 in Albania. Ann. Medit. Burns Club, 7: 5-7,
1994.
- Tejerina C., Reig A., Codina J. et al.: An epidemiological
analysis of burn patients hospitalized in Valencia, Spain, during 1989. Burns, 18: 15,
1992.
- Sowemimo G. 0.: Burn injuries in Lagos. Burns, 9: 280-3,
1982.
- El Danaf A., Alshlash, Filoppos P. et al.: Analysis of 105
patients admitted over a 2-year period to a modem burns unit in Saudi Arabia. Burns, 17:
62, 1991.
- Bang R.L., Mosbah K.M.: Epidemiology of burns in Kuwait.
Burns, 14: 194-200, 1988.
- Muir 1. F. K., Barclay T.L., Settle J.A. D.: "Burns
and their treatment" (3rd edition). Butterworth, 1987.
- Perro G., Bourdarias B. et al.: Analyse 6pid6miologique de
2000 br6l6s hospitalis6s ~ Bordeaux entre 1987 et 1994. Ann. Burns and Fire Disasters, 9:
131-8, 1996.
- Bouayad A.R., Benhamia A.: Epidemiology of burns in
Algeria. Burns, 5: 204-5, 1978.
- Mazla C.N., Misgar M.S. et al.: Study of burns in Kashmir.
Burns, 9: 180-3, 1982.
- El-Muhtaseb H., Qaryoute S., Raheb S.A.: Burns injuries in
Jordan: a study of 338 cases. Burns, 10: 116-20, 1984.
- Yoshioka T., Ohashi H., Sugimoto H.: Epidemiological
analysis of deaths caused by burns in Osaka, Japan. Burns, 8: 414, 1982.
- Josep T.P., Douglas B.S.: Childhood burns in south
Australia: a socio-economic and aetiological study. Burns, 5: 335- 42, 1978.
- Word E.L., Meacher D.E. et al.: Epidemiology of burn
injuries in a rural community. Burns, 5: 343-8, 1978.
- Charosia A.R.: Motality from burns in developing countries.
Burns, 9: 184, t982.
- Hegazi M., Ibrahim E.: The pattern and outcome of burn
injuries at a burn unit in Saudi Arabia: retrospective analysis of 501 consecutive
patients. Ann. Saudi Medicine, 11: 3,1991.
- Napoli B., D'Arpa N., Masellis M.: Epilepsy and burns. Ann.
Medit. Burns Club, 5: 155-9, 1992.
| This paper was received on 7 August 1998 Address correspondence to: Dr. A.R.S. El-Gallad
Burn Unit, Aljala Hospital, Benghazi, Libya |
|