| Annals of Burns and Fire Disasters - vol. XI - n. 4 - Deceinber
1998
SEVERE BURNS IN CHILDREN IN THE LAST FIVE YEARS IN ALBANIA
Belba G, Perna L, Belba M, Isaraj S, Mingomataj L.
Mother Teresa Clinic of Burns and Plastic Surgery
University Hospital Centre, Tirana, Albania
SUMMARY. This
is an epidemiological and statistical survey of the occurrence of severe burns among
children in Albania in the last five years. The patients taken into consideration were
burned children from all parts of the country as well as from the capital of Albania,
admitted to and treated in the intensive care unit of the Clinic of Burns and Plastic
Surgery in the University Hospital Centre of Tirana, Albania. Special attention is paid to
the body area where the burns occurred, as compared with other burned patients admitted to
our ICU, the age groups most subject to severe burn injury, sex distribution, and the site
of the accident. In the five-year period there was a prevalence of 10-20% and 20-30% BSA
burns. The causative agents (flame, hot water and liquids, electric current, chemicals)
were studied in relation to the percentages of the burns and their location in particular
body areas. The treatment protocol is described, and in particular the resuscitation
phase, local treatment, general therapy, and the possible complications due to burn shock
or sepsis. Total mortality figures are presented, with the main causes of death. In
addition to cases in which epithelialization was spontaneous, the plastic surgery
approaches adopted to treat severely burned children are described. The application and
combination of different surgical stages, i.e., eschar excision and meshed skin grafting
at the appropriate time, are% introduced as a possible successful management option. The
data obtained underline the importance of propaganda campaigns for the prevention of
severe burns in children.
Introduction
The reasons why we decided to study severe
burns in children were multiple, but what really prompted our decision was the observation
that 93 severely burned children were admitted to our intensive care unit in the first six
months of 1998, corresponding to 79% of all patients treated there during that period.
Because of a prolonged transition from one social system to another, with profound
reflections on the political, economic and social life of our people, there has been a
constant increase in the incidence of severe burns in children compared with past years.
There has been an uncontrolled demographic displacement of the population, with people
moving from the villages towards larger centres, and many of the families and social
groups involved live in conditions below the average standard of living.
On the basis of the evidence provided by this group of burn patients, this paper aims to
help promote the prevention of burns by making people aware of the serious danger that
burns represent for children. The objectives of the study are twofold, and they will
become clear with the analysis of the clinical material.
First, we will present statistical and epidemiological data regarding:
- the diseases treated in our ICU during the five-year period
- the occurrence of severe burns in children
- the distribution of burns in di ' fferent age groups
- the site and causative agent of-the accidents
- the location, size of burn, and patient condition on
admittance
Secondly, we will survey the mortality
rate from a number of viewpoints:
- shock and sepsis
- complications
- the various causative agents and the BSA burned
- the different age groups and the overall mortality rate
Material and method
All severely burned children admitted to
our ICU who fulfilled the relevant criteria were included in the study, which extended
over the years 1993-1997.
The contingent consisted of 560 children, out of the total number of 834 patients treated
in the ICU of the Clinic of Burns and Plastic Surgery in the University Hospital Centre,
Tirana, Albania.
The study is of an epidemiological -statistical nature, with the clear clinical objective
of promoting the improvement of our present protocols for treating severely burned
children.
Results
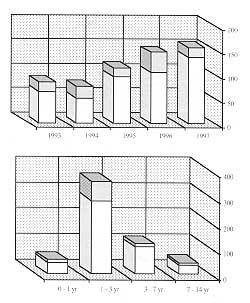
Beginning in 1993, as shown in Table I, we
observed a galoping increase in the incidence of severe burns in children, which was twice
as high in 1997 as it was in 1993. No important increase was recorded in the number of
burned adults or elderly patients. Burned children constituted 67% of our burn cases.
| Year |
Burns
+ (Burns + Trauma) |
Others |
Total |
| Children |
Adults |
Elderly |
Total |
1993 |
85 |
42 |
9 |
136 |
6 |
142 |
1994 |
65 |
36 |
9 |
110 |
7 |
117 |
1995 |
113 |
36 |
13 |
162 |
8 |
170 |
| 1996 |
142 |
42 |
9 |
193 |
2 |
195 |
1997 |
155 |
59 |
19 |
233 |
10 |
243 |
Total |
560 |
215 |
59 |
834 |
33 |
867 |
|
Table I -
Diseases treated in ICU in last five years |
|
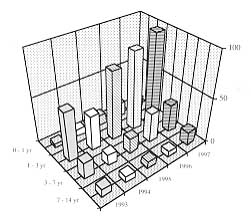
With regard to the
distribution of burns according to age group (Table 11), 63.4% of the cases
occurred in children in aged 1-3 yr, a stage in life that is notorious for impulsive
behaviour and excessive curiosity. Boys slightly prevailed over girls, with a
male/female ratio of approximately 1.2A. In 304 cases (54.4%) the children came from
villages, the rest, i.e., 256 cases (45.6%), coming from towns. Ninety-four point four per
cent of the accidents took place in the home.
|
Table II
- Burns in different age groups |
| Year |
Age Group |
| 0-1 yr |
1-3 yr |
3-7 yr |
7-14 yr |
Total |
| 1993 |
4 |
55 |
18 |
8 |
85 |
| 1994 |
8 |
39 |
12 |
6 |
65 |
| 1995 |
12 |
76 |
17 |
8 |
113 |
| 1996 |
16 |
87 |
33 |
6 |
142 |
| 1997 |
11 |
98 |
31 |
15 |
155 |
| Total |
51 |
355 |
111 |
43 |
560 |
| Percentage |
9.1 |
63.4 |
1 199 |
7 6 |
100 |
|
|
The high rate of
domestic burns reflects the inappropriate care children receive at home, compared with the
care provided at pre-school and school institutions.
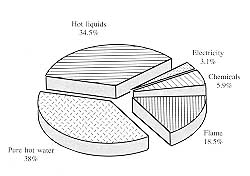
Table III contains details of the distribution of burns according to the causative
agent in different age groups.
|
Table III -
Causative agent of burns |
Causative
agent |
Age Group |
% |
Number
of deaths |
Mortality
rate |
0 - I yr/
deaths |
I - 3 yr/
deaths |
3 - 7 yr/
deaths |
7 - 14 yr/
deaths |
Total |
| Flame |
14/5 |
44/15 |
29/2 |
17/6 |
104 |
18.5% |
28 |
26.9% |
Pure hot
water |
20/3 |
149128 |
40/6 |
512 |
214 |
38% |
39 |
18.2% |
Other hot
liquid |
15/2 |
134/23 |
34/2 |
11 /1 |
194 |
34.5% |
28 |
14.4 % |
| Electricity |
1/0 |
9/3 |
t/O |
4/0 |
15 |
3.1% |
3 |
26k |
| Chemicals |
I / 1 |
19/5 |
7/2 |
6/0 |
33 |
5.9% |
8 |
1 1 |
| Total |
51/ 11 |
355/74 |
111/12 |
43/9 |
560 |
|
106 |
18.9% |
|
|
The commonest
causative agents were hot water (38% of cases) and other hot liquids (34.5%), followed by
flame (18.5 %). Electrical and chemical burns represent respectively 3.1% and 5.9% of the
cases. Table III also shows the relation between the causative agent and mortality,
which was higher in flame burns than in scalds, but with no marked difference between
flame burns and chemical burns. The number of deaths is higher in children aged 1-3 yr,
with hot water as the most frequent causative agent. These figures are explained by the
ratio of 149 scalds treated to 28 fatal outcomes in this age group.
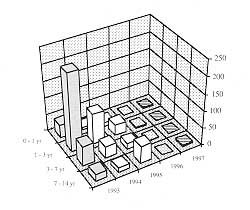
The principal criterion of admittance to our ICU is the extent of the burn. Children are
admitted if they present deep 2nd- or 3rd-degree burns in more than 10% BSA. When wounds
were located in critical areas, the threat to the child's life was greater, especially at
the age of 0-1 yr. Burns involving 10-20% BSA prevailed (Table IV), these
constituting 62.9% of our cases - again, children aged 1-3 yr old were the most frequently
involved, with 231 cases. Deaths, although rare, nevertheless occurred even in children
with up to 20% burns (8.5%). The death rate increased progressively with the increase in
burn size.
|
Table IV
- TBSA burns |
| |
Age group |
% |
Number
of deaths |
Mortality
rate |
0 - 1 yr/
deaths |
1-3 yr/
deaths |
3 - 7 yr/
deaths |
7 - 14 yr/
deaths |
Total |
| 10-20% |
39/3 |
231/27 |
60/0 |
21/0 |
351 |
62.9% |
30 |
8.5% |
| 21-30% |
9/5 |
89/26 |
32/3 |
1312 |
143 |
25.5% |
36 |
25.1% |
| 31-50% |
0/0 |
33/19 |
18/8 |
5/3 |
56 |
10% |
30 |
53.6% |
| 51-60% |
1 /l |
2/2 |
1 /1 |
010 |
4 |
0.7% |
4 |
100% |
| > 60% |
212 |
0/0 |
010 |
4/4 |
6 |
1.2% |
6 |
100% |
| Total |
51/11 |
355/74 |
111/12 |
43/9 |
560 |
|
|
8.90% |
|
|
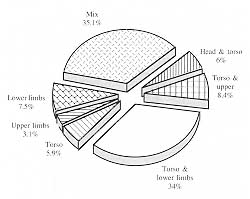
Burns were generally
located in combined areas of the body, e.g. the torso and lower limbs, as was the case in
34% of the cases (Table V). The classic diagnosis was "scald of the hips,
buttocks and thighs", sustained when the child accidentally stumbled and fell into a
hot liquid. Such injuries usually extended over the genital area, rendering management
even more complicated.
Leaving the treatment protocol for discussion in a later part of the paper, we will now
report on mortality, with an analysis of various different factors. Thanks to adequate
fluid resuscitation and appropriate follow-up in the initial phase, only 0.9% of the
children died within the first 48
|
Table V
- Location of burns |
| |
Head &
torso |
Torso &
upper
limbs |
Torso &
lower
limbs |
Torso |
Upper
limbs |
Lower
limbs |
Mix |
Total |
| 1993 |
6 |
13 |
33 |
3 |
5 |
5 |
20 |
85 |
| 1994 |
6 |
4 |
20 |
6 |
0 |
4 |
25 |
65 |
| 1995 |
9 |
10 |
44 |
5 |
2 |
15 |
28 |
113 |
| 1996 |
7 |
9 |
46 |
8 |
4 |
8 |
60 |
142 |
| 1997 |
6 |
11 |
48 |
11 |
7 |
10 |
62 |
155 |
| Total |
34 |
47 |
191 |
33 |
18 |
42 |
195 |
560 |
Percentage |
6% |
8.4% |
34% |
5.9% |
3.1% |
7.5 % |
35.1% |
|
|
|
h, i.e., during the
shock phase, with a constant fall in the number of deaths in consecutive years. Mortality
was high (40%) in septic patients, as a consequence of severe infections caused by S. aureus
and gram-negative germs like P. aeruginosa, Klebsiella, Proteus, etc.
Fifty-nine out of the 560 severely burned children (10.5%) developed complications, of
which the commonest were bronchitis, bronchopneumonia, pneumonia and pleurisy. Cardiac and
cerebral complications were less frequent. The death rate of patients with complications
was 37%.
Among the causes of death, septic shock complicated by acute renal failure took first
place, accounting for 93.4% of all deaths. Haemorrhagic stress ulcer and multiple organ
failure accounted for 3.7% and 2% of deaths respectively.
Sixty per cent of the deaths occurred within the first week post-burn, 27% within two
weeks and 12.1% after the second week. A synthesis of mortality rate data in the different
years and age groups is presented in Table VI. The overall mortality rate was
18.8%.
The average hospital stay was 10.1 days (6.8 days in children who died).
|
Table VI
- Mortality rate in severely burned children |
Year |
Age Group |
Total |
Mortality |
0 - 1 yr/
deaths |
1 - 3 yr/
deaths |
3 - 7 yr/
deaths |
7 - 14 yr/ |
1993 |
4/2 |
55/14 |
1811 |
8/1 |
85/18 |
21% |
1994 |
8/3 |
39/10 |
12/3 |
6/5 |
65/21 |
32.3% |
1995 |
12/1 |
76/12 |
17/2 |
8/0 |
113115 |
13% |
1996 |
16/3 |
87/26 |
3313 |
6/2 |
142/34 |
23.9% |
1997 |
11/2 |
98/12 |
31/3 |
15/1 |
155/18 |
11.6% |
Total |
51/11 |
355/74 |
111/12 |
43/9 |
560/106 |
|
Mortality |
21% |
20.8% |
10,9% |
20.9% |
Overall
mortality
18.3% |
|
|
Discussion
In the majority of cases (71.9%), the
burned children came to our clinic straight from the accident site. This might imply that
they received qualified medical care immediately, but on the other hand a great number of
patients can be regarded as delayed cases because the time interval between the accident
and initiation of treatment was rather protracted owing to transport difficulties.
Eighteen per cent of the children came from district hospitals, but although they were
already being treated they should be regarded as delayed patients, because transfer was
effected after signs and symptoms of sepsis were established. The most difficult
contingent to deal with wasthat of children treated as out-patients at incompetent centres
where they were inadequately treated for some long time before being sent on to us, when
their general condition had deteriorated.
The condition of the children on admittance was estimated to be severe in 73.4% of cases
and very severe in 26.6%. This latter estimation was made in patients with profound
haemodynamic alterations and marked irregularities in fluids, electrolytes, acid-base
balance, etc.
Fluid resuscitation was performed using the Carvajal formula. We gave greater amounts of
fluids, generally consisting of Ringer's lactate or 0.9% saline solutions, when the burns
were located in critical areas. The same formula guided resuscitation in delayed arrivals,
but the amounts given in these cases were intended to maintain urinary output at a level
of 1 ml/kg/h, in order to avoid pulmonary overload. Colloids were usually given after the
sixth hour post-burn, following the initial fluids. However, in cases that seemed
resistant to crystalline solutions, with a poor clinical response, colloids were initiated
earlier.
Antibiotics were administered only after the second day post-burn. Our treatment of choice
is a combination of an aminoglucoside (mainly amikacin) with a thirdgeneration
cephalosporin. This treatment was continued for 10-15 days. After the second week,
protection from infection was implemented using a first-generation cephalosporin combined
with an anti-staphylococcal agent.
The above schemes are based on the microbial load of the ICU environment, as found by the
results of blood cultures and antibiograms. Blood transfusions were performed, depending
on the blood count, when the haematocrit was lower than 30% and haemoglobin less than 8
gl%. Treatment was completed with electrolytes, antacids, antifungals, analgesics and
nutritional supplements.
The surgical treatment protocol was initiated with the first debridement of the burn
wounds, which was carried out under intravenous anaesthesia with ketamine, followed by the
closed method using Betadine 10%. After the third day, at the end of the exudation phase,
we applied silver sulphadiazine 1% until all the burned tissues separated. If the burn was
deep 2nd-degree and the wounds showed epithelial islands, epithelialization was promoted
by the application of antibiotic-impregnated fine mesh gauze, phytostimulin or mitosyl. In
3rd-degree wounds the surgical protocol varied in relation to the size and the causative
agent of the burn, as follows:
- In 3rd-degree burns of less than 10% BSA we performed late
excision after the 7th-8th day and grafted them in a second procedure.
- In 3rd-degree burns of more than 15% BSA we performed late
excision and partial grafting, covering functional areas with autologous skin, either in
sheets or meshed by 2. Later, in a second and not infrequently a third stage, the wounds
were covered completely with grafts passed through a no. 4 or 6 mesher.
- In electrical burns, as soon as the child's general
condition permitted, immediately after the shock phase, we performed early excision or
limb amputations as necessary.
- In chemical burns our mainstay of management was early
excision on the fourth or fifth day postburn, with re-estimation of the wound after some
days followed by a further excision procedure in separate areas and grafting at the
appropriate moment.
With clinical-biochemical stabilization -
generally after the first surgical procedure - the child's condition began to ameliorate
towards a safer prognosis. At this point a general consultation of our staff decided
whether the child was to remain in the ICU or be transferred to other wards in our clinic
for completion of treatment.
Conclusions
Statistical-epidemiological papers
also take into account the clinical aspect of the treatment of the cases studied as well
as anticipating scientific research. Their importance is even greater when the subject
considered is the incidence of certain diseases in different social groups, especially
when they encompass the entire population of a country, so that the results are available
for comparison with those of other countries.
Our series of 560 cases is sufficient to provide data that can be statistically processed.
As in many other countries` burns in children aged 1-3 yr continue to be a problem, the
majority being due to domestic scalds."-'' Flame burns are the second most frequent
type in our country, as elsewhere, while electrical and chemical burns, though rare,
require special care.
The frequent occurrence of burns to our children in the home is comparable with data from
most European countries, adding further evidence to the importance of prevention
campaigns. Our data indicate a relatively high mortality rate, but there is also a clear
tendency for reduction in consecutive years. In spite of the difficulties we face, with
tremendous limitations in materials and equipment, mortality - both in the different age
groups and as regards overall mortality - is comparable with that reported in countries at
a similar stage of economic development. Much still remains to be done for our results to
approach those of other European clinics, which currently report death rates much lower
than ours.
In Albania, there is one disturbing trend. Compared with the findings of another study we
performed,` there is a clear increase in the number of severely burned children, contrary
to findings elsewhere. A great deal still remains to be done in the field of prevention
and treatment.
With regard to prevention and its social aspect we must:
- promote greater awareness of the particular dangers that
burns pose to children
- educate social groups and families living in disadvantaged
conditions with regard to this issue
- encourage public institutions to increase the number of
pre-school and school centres and to improve their work in the field of child health care,
including burn prevention
- organize specialized medical teams for the monitoring of
the health status of demographically mobile social groups
Clinically we must:
- strengthen aseptic measures in order to enhance protection
from staphylococcal and Pseudomonas infection
- perform excision, with an individual approach in each case,
avoiding any tendency towards extreme standardization
- create special units within ICUs for the management of
severely burned children
RESUME. Les Auteurs
présentent une analyse épidémiologique et statistique qui étudie les brûlures
sévères des enfants en Albanie dans les années 1993-1997. Les enfants, qui provenaient
de toutes les régions du pays, y inclus la capitale, ont été hospitalisés dans le
Centre de Réanimation de la Clinique des Grands Brûlés et Chirurgie Plastique du Centre
Hospitalier de l'Université de Tirana (Albanie). Les Auteurs ont consideré en
particulier le lieu où l'accident a eu lieu, l'âge des patients, le sexe et la zone
corporelle atteinte. L'analyse des résultats démontre la prévalence des brûlures de
10-20% et de 20-30% de la surface corporelle. Les Auteurs considèrent en outre les agents
étiologiques qui ont causé les accidents (les flammes, l'eau et les liquides chaudes, le
courant électrique et les substances chimiques) en relation avec le pourcentage de la
surface corporelle brûlée et les zones particulières intéressées. Le protocole du
traitement est décrit, avec un intérêt particulier pour la phase de la réanimation, le
traitement local, le décours de la maladie et les complications dues au choc de la
brûlure ou à la sepsis. Les Auteurs présentent les données sur la mortalité totale et
les causes principales de la mort. A part les cas d'épithélialisation spontanée, ils
présentent leurs expériences dans le champs de la chirurgie plastique dans le traitement
de l'enfant brûlé. Ils utilisent l'excision de l'escarre et la greffe du type mesh
graft, comme option possible dans la gestion de la maladie. En conclusion, les Auteurs
répètent l'importance de la propagande dans la prévention des brûlures sévères des
enfants.
BIBLIOGRAPHY
- Hendrickx A., Boeckx W.: Burn campaigns in Belgium for
children under the age of five years. Ann. Burns and Fire Disasters, 10: 1215,1997.
- Benito Ruiz J., Navarro Monzonis A., Montana Vizcaino J.,
Mena Yago A,, De La Cruz Ferrer L.I., Mirabet Ippolito V.: A study of burns in children,
Ann. Medit. Burns Club, 4: 79-83, 1991.
- Tryfonas G., Gavopoulas S., Limas C., Zioutis I., Violaki
A., Klokkaris A., Fragos E., Grigoriadis G.: Burns in childhood - a tenyear experience in
management. Ann. Medit. Burns Club, 5: 15-17, 1992.
- Ahouangbevi A,, James K., Ayite A.: Epid6miologie des
br6lures de 1'enfant en milieu togalais. Ann. Medit. Burns Club, 5: 8-10, 1992.
- Rojas Z.J., Carrasco T.R., Comejo A.E., Cortes P.L.:
Epidemiology of burns by fireworks in children. Ann. Medit. Burns Club, 7: 1846, 1994.
- Napoli B., D'Arpa N., Gullo S., Masellis M.: Epidemiology,
clinical treatment and therapy in electrically burned children. Ann. Medit. Burns Club, 7:
188-93, 1994.
- Diakov R., Hadjiiski 0., Atanassov N., Argirova M.: Etude
des brûlures chez les enfants admis au Centre des Brûlés à Sofia sur une periode de
six ans (1988-1993). Ann. Medit. Burns Club, 8: 135-9, 1995.
- Zaidi M.M., Abussetta A.A., Franka M.R, Shahata G., Traikov
E., Liyang L.: Management of severely burned patients - a study of 684 severely burned
patients, admitted in the last six years to the Burn and Plastic Surgery Centre, Tripoli,
Libya. Ann. Burns and Fire Disasters, 9: 3-7, 1996.
- Reig A., Tejerina C., Baena P., Mirabet V.: Epidemiological
study of scalding in children. Ann. Medit. Burns Club, 6: 157-60, 1993.
- Fadaak H., Fawzy S., EI-Fayomy S., At-Kurashi N., Esawi 0.,
Nada I.: Admission and pattern of burn injuries at a new burn unit at Unayzah, Qassim,
Saudi Arabia. Ann. Burns and Fire Disasters, 9: 73-8, 1996.
- Zaidi M.M., Abussetta A., Brogowski A., Agrawal P.L.,
Franka MR.: Analyses of burned children treated in the Burns and Plastic Surgery Centre,
Tripoli, Libya, in the year 1992. Ann. Medit. Burns Club, 6: 217-21, 1993.
- Boukind E.H., Chafiki N., Bahecar N., Alibou F., Terrab S.,
Boumzebra D., Zerouali O.N.: Les brfil6s: profit 6pid6mologique et 616ments de prevention
~ propos de 1499 patients hospitalis6s A l'Unit6 des Br6l6s de Casablanca, Maroc. Ann.
Medit. Burns Club, 7: 57-61, 1994.
- Perro G., Bourdarias B., Cutillas M., CastMe J.C., Sanchez
R.: Analyse épidémiologique de 2000 brûlés hospitalisés à Bordeaux entre 1987 et
1994. Ann. Burns and Fire Disasters, 9: 131-7, 1996.
- Lindblad B.E., Jerkelson C.J.: Domestic burns among
children. Burns, 16: 254, 1990.
- Boukind E.H., A., Chlihi N., Alibou F., Terrab S., Bouchta
A., Bahechare N., Zerouali O.N.: Etude de la mortalite par brOlure A propos de 414 cas de
d6c&s. Ann. Burns and Fire Disasters, 8: 1959, 1995.
- Gupta M.: Pediatric burns in Jaipur, India - an
epidemiological study. Burns, 18: 63, 1992.
- Oluwasanmi J.O.: Burns in Western Nigeria. Brit. J. Plast.
Surg., 14: 216-23, 1986.
- Belba G.J., Andrea A., Dauti I., Osmani X.H., Cano N.,
Perna L.: Some epidemiological data regarding burn patients treated during 1992 in
Albania. Ann. Medit. Burns Club, 7: 5-7, 1994.
- Haberal M., Uqar N., Bayraktar U., Oner Z.: Analysis of
1005 burn patients treated in our centre. Ann. Medit. Burns Club, 6: 73-5, 1993.
- Genco F., Favasuli R., Pagano R., Golotta R.: Paediatric
burn injuries in the Calabria area of Italy. A study of 383 patients. Ann. Burns and Fire
Disasters, 9: 201-3, 1996.
This paper was presented at the
Fourth Conference on
Burns and Fire Disasters held in Athens in October 1998.Address correspondence to: Prof. Gjergji Belba
Mother Teresa Clinic of Burns and Plastic Surgery University Hospital Centre
Tirana, Albania. |
|