| Annals of Burns and Fire Disasters - vol. Xl - n. 4 - December 1998
ELECTRICAL BURNS IN THE BENGHAZI URBAN AREA
EI-Gallal A.R.S., Yousef S.M.
Plastic and Burn Unit, Al-Jala Hospital,
El-Arab Medical University, Benghazi, Libya
SUMMARY. Between January 1988
and December 1997, a total number of 389 patients aged between 2 and 58 years with true
electrical burns were treated in the Burn Unit of Aljala Hospital in Benghazi, Libya.
Benghazi is a growing city that has upcoming industrial units in the suburbs, and the
hospital serves not only the city but also the surrounding villages and receives all
referral cases from the eastern part of Libya. Thirty-eight patients sustained
high-voltage electrical injuries while in the other 351 the burns were low-voltage.
Initial resuscitation was employed in most of the patients; we also carried out
appropriate urgent surgery whenever required. Despite the medical and surgical management,
nine patients with high-voltage and seven with low-voltage injury succumbed to their
injuries. Our study showed that electrical injury remains a formidable problem with
significant morbidity. It is therefore advocated that an appropriate preventive plan
should be drawn up and applied.
Introduction
A true electrical burn is one of the most
devastating injuries to be seen in emergency departments, and is attended by high
morbidity and mortality rates. We report here on aspects of true electrical burns seen in
A1jala Hospital, which serves the population of the Benghazi urban area, Eastern zone,
Libya. Over a period of ten years (19881997), electrical burned patients constituted 7.4%
of all admissions to our Burn Unit. Only 4.4% of the patients had sustained true
electrical burns with actual contact with live electric wire (flash and heat burns were
excluded). This paper reviews these cases. The emphasis is on the pattern and outcome of
the injuries with reference to our management.
Patients and methods
The medical records of all the patients
admitted to our Burn Unit with true electrical burns between January 1988 and December
1997 were thoroughly reviewed with reference to the following variables: age, sex,
occupation, site of accident, tension of the current (voltage), clinical presentations,
surgical procedures, and outcome. Our specific management for electrical injury includes
immediate cardiorespiratory resuscitation and administration of intravenous fluids (plasma
and Hartmann's solution). In the presence of myoglobinuria, we encouraged osmotic diuresis
by infusing an adequate amount of Ringer's lactate (Hartmann's) solution and mannitol 20%
(I g/kg), in addition to sodium bicarbonate solution, with the aim of obtaining an
alkaline-urine output of 1.5-2 ml/kg/h. Povidone-iodine (Betadinel) and silver
sulphadiazine (Flamazinel) were the main items used locally for dressing the burn wounds.
Required surgical procedures were usually carried out urgently after being appropriately
selected for given patients.
Results
Out of 8851 burned patients, 655 (7.4%)
presented with electrical burns during the 10-year period. 389 patients (4.4%) - 149 of
whom had been referred from other peripheral hospitals - had sustained real electrical
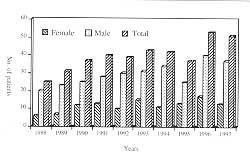
burns. The pattern of annual admission is shown in Fig. 1. The annual male to female ratio
was variable but it was always greater than 2 to 1. Thirty-eight patients (9.8%), one of
them a 26-year-old female, were electrocuted by high-voltage line (> 1000 V); the
majority were electricians who had ignored safety precautions. With regard to the other
351 patients (90.2%), of whom 248 were male and 103 female, the injuries were due to
low-voltage current. Two hundred and two patients (51.9%), including 125 pre-school
children, suffered their injuries at home (102 males and 100 females) (Table I).
Site of
accidents |
Type of injury and sex |
% |
|
|
|
Outdoors |
|
|
183
4 |
48.1% |
At home |
|
|
102
100 |
51.9% |
Total |
|
|
285
104 |
100% |
| % |
9.8% |
90.2% |
100% |
|
|
Table 1 -
Distribution of patients by type and place of injury |
|
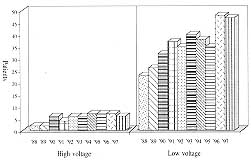
The annual frequencies of
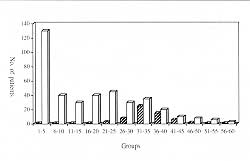
high- and low-voltage injuries are shown in Fig. 2, and distribution by age in Fig.
3. The high-voltage injuries all occurred in adult patients, while low-voltage
injuries predominated in the younger age groups.
The mean age (± SD) of patients with low-voltage injuries was 16.4 yr (± 13.8) (range
2-58 yr), and with high-voltage injuries 34.5 yr (± 5.8) (range 2247 yr). Further
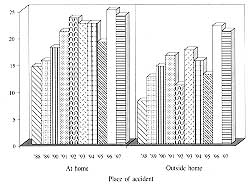
analysis of the annual frequency of low-voltage injury in relation to the place of
accident (at home or outdoors) is shown in Fig. 4.
 |
 |
| Fig. 1
- Annual admission. |
Fig.
2 - Annual frequency of low- and high-voltage injuries. |
 |
 |
| Fig.
3 - Distribution of low- and high-voltage injuries by age. |
Fig.
4 - Annual frequency of low-voltage injuries by place of accident. |
|
The clinical presentation of our patients
was variable. Most of those with high-voltage injuries presented with shock and loss of
consciousness. One patient sustained spinal fracture, while another one had shoulder
dislocation. Six patients developed acute renal failure around the third day post-injury.
Confusion, dizziness and various types of cardiac arrhythmia other than conduction
disorders were frequently recorded in low-voltage injuries.
The extremities were most commonly affected in both types of injury, the upper limbs being
more frequently involved (Table II). The mean (± SD) total burned surface area was
9.7% (± 9.2) and ranged between 0.25 and 55%.
Body
regions |
No. of patients |
| H.V. |
(%) |
L. V. |
(%) |
Both types |
(%) |
Upper extremities |
35 |
(92.1) |
327 |
(93.2) |
362 |
(93.1) |
Head and face |
11 |
(29.0) |
43 |
(12.3) |
54 |
(13.9) |
Neck |
3 |
(7.9) |
8 |
(2.3) |
11 |
(2.8) |
Chest |
14 |
(36.8) |
23 |
(6.6) |
37 |
(9.5) |
Abdomen |
6 |
(16.8) |
2 |
(0.7) |
8 |
(2.1) |
Back |
8 |
(21.1) |
1 |
(0.3) |
9 |
(2.3) |
Perineum |
2 |
(5.3) |
0 |
(0.0) |
2 |
(0.5) |
Lower extremities |
29 |
(76.3) |
209 |
(59.5) |
28 |
(61.2) |
H.V. = High voltage
L.V.= Low voltage |
|
| Table II - Distribution of number and percentage of patients
by type of injury and body area involved |
|
Overall, high-voltage current caused very
deep and extensive tissue damage (Fig. 5), while low-voltage current resulted
mainly in full-thickness and deep dermal burns, although significant tissue damage was
occasionally observed (Figs. 6, 7). In addition, some patients whose clothes caught fire
suffered extensive flame burns.
 |
Fig. 5
- Very extensive tissue damage seen in a high-voltage injury. |
 |
 |
| Fig. 6 -
Severe hand injury in child caused by a low-voltage current. |
Fig. 7 -
Multiple deep burns and below-elbow amputation after lowvoltage injury. |
|
Considering all admissions, there were 16
deaths (4.1%). Nine of these occurred among patients with highvoltage injuries (23.7%):
four deaths within a few hours of admission were due to persistent serious arrhythmia and
cardiac arrest, three to septicaemia, DIC and multisystem failure, and two to acute renal
failure. There were seven deaths among the 351 patients with low-voltage injury (2%); six
of these were children aged under 12 yr, while the seventh was a 56-year-old female. Five
patients sustained extensive flame burns; their deaths were due to the consequences of
burn sepsis. Three of the five were referred to our hospital some days after injury, of
whom two presented established acute renal failure and one mental retardation (Down
syndrome). Of the remaining two deaths the 56-year-old diabetic female developed severe
respiratory complications, while the other patient developed gramnegative septicaemia and
multisystem failure.
Twenty-three patients with high-voltage injuries and 273 with low-voltage injuries were
operated upon. Seventyone patients with low-voltage injuries were treated conservatively.
The surgical procedures and their frequencies are shown in Table III, together with
an analysis of the group subjected to amputation.
| Type of surgery |
No. of patients |
Frequency of surgery |
| Skin grafting |
285 |
304 |
| Flap surgery |
56 |
64 |
| Debridement |
196 |
216 |
| Escharectomy/Fasciotomy |
39 |
43 |
| Amputation (total) |
53 |
71 |
Forequarter
Above elbow
Below elbow
Hand (partial)
Below knee
Foot (partial)
Fingers and toes |
3
9
3
1
7
6
42 |
|
| Table III - Number of patients operated on and
frequency of each surgical procedure |
|
The most significant complications were
septicaemia in 48 patients, myoglobinuria in 13, acute renal failure in 8, DIC in 7,
multisystem failure in 4, respiratory complications in 3, wound infection in 124, delayed
healing in 42 (wound not dry by day 14 post-operation or subsequent breakdown), spinal
neuropathy (motor) in 2, and peripheral main nerve injury in 56. One patient developed
bilateral cataract 6 months post-injury.
Six of our high-voltage group, of whom four were nonLibyan expatriates, discharged
themselves against medical advice in order to be treated elsewhere.
Discussion
The trends of both types of injury in our
region differ from those reported elsewhere in the literature.` This could be due to many
factors, such as progress in the country's industrial and agricultural development, lack
of attention because of crowded living condition (large families living in flats), rapid
urbanization, and the community's sociocultural transformation.
It is clear that the incidence of both high- and lowvoltage injuries increased over the
years. Low-voltage injuries outnumbered high-voltage injuries, in contrast with other
findings."` This is evidently due to the considerable number of domestic accidents
and paediatric involvement.
In our study, the incidence of low-voltage domestic injuries (57.55% = 202/351) and of
industrial injuries (42.45% = 149/351) was consistent with other results.' In our series,
however, children were involved more frequently.
While neglect of industrial safety precautions was the principal cause for high-voltage
injuries in most of our cases, the main causes of low-voltage injuries were carelessness,
improper use and negligence. Other causes were occasionally recognised.
Regarding factors modulating the severity of injuries, such as type and strength of
current, and time and nature (resistance) of contact, the clinical presentations of our
patients differed little from those reported elsewhere. " None of our patients
suffered any involvement of internal organs.
The two types of true electrical burns have a different epidemiology and vary considerably
in their clinical presentation and outcome, while instead electrical injury mechanisms` `
remain the same and are applicable for both types. It is therefore reasonable to treat
both types of injuries on the basis of the same management principles, although care must
of course be individualized.
In severe injuries, it is well established that any reduction in time lost before starting
adequate resuscitation, surgical decompression and appropriate debridement will have a
favourable effect on morbidity and mortality." 12,13 Hence our management is based
upon instant cardiovascular resuscitation and renal support, in addition to the
application of what we would prefer to call an 11 urgent appropriate surgical
approach" rather than an aggressive surgical approach,' whenever it is required. The
outcome of delay in treatment can be lethal, as was seen in three of our paediatric
patients who succumbed to their injuries.
Finally, we believe that the results of this study, including the epidemiological trends,
are not unique to our community, and could be expected in other similarly developing
societies. Moreover, the complexity of the injuries, the urgent need for versatile
management, and the potentially catastrophic complications make such injuries a genuine
health hazard. Proper educational programmes must therefore be designed and implemented in
order to reduce the frequency of this devastating form of injury in our developing
societies.
RESUME. Entre janvier 1988
et décembre 1997 les Auteurs ont traité 389 patients atteints de brûlures électriques
véritables âgés de 2 à 58 ans chez l'unité des Brûlures de l'Hôpital AI-jala à
Benghazi, Libye. Benghazi est une cité croissante avec de nouvelles zones industrielles
en banlieue. L'Hôpital AI-jala sert non seulement la cité mais aussi les villages
voisins et reçoit tous les cas provenant de la région orientale de la Libye. Trente-huit
patients ont été atteints de brûlures électriques à haute tension et les autres 351
patients ont subi des brûlures à basse tension. La plupart des patients ont reçu la
réanimation immédiate et les Auteurs ont effectué une "chirurgie appropriée
urgente", selon les nécessités. Malgré la gestion médicale et chirurgicale les
Auteurs ont constaté le décès de neuf patients atteints de lésions à haute tension et
sept à basse tension. L'étude a démontré que les lésions électriques restent un
grave problème accompagné d'une morbidité significative. Les Auteurs soulignent
l'importance de la préparation d'un projet préventif approprié qu'il faut appliquer
avec soin.
BIBLIOGRAPHY
- Napoli B., D'Arpa N., Gullo S., Masellis M.: Epidemiology,
clinical treatment and therapy in electrically burned children. Ann. Medit. Burns Club, 7:
188-93, 1994.
- Hadjiiski 0., Argirova M.: Observation clinique des
brûlures à haut voltage. Ann. Burns and Fire Disasters, 9: 13-17, 1996.
- Lochaitis A., fliopoulou E., Poulikakos L.G., Asfour S.:
Electrical burns: A survey of 24 cases. Ann. Medit. Burns Club, 5: 75-7, 1992.
- Haberal M.: Electrical burns: A five-year experience. J.
Trauma, 26: 103-9, (year not provided).
- Moran K.T., Munster A.M.: Low voltage electrical injuries:
The hidden morbidity. J. Royal Coll. Surg. Edinburgh, 31: 227-8, 1989.
- Holliman CT, Saffle J.R., Kravitz M., Warden G.D. et al.:
Early surgical decompression in the management of electrical injuries. Am, J. Surg., 144:
733-9, 1982.
- Parshley P.F., Kilgore J., Pulito J.F. et al.: Aggressive
approach to the extremity damaged by electric current. Am. J. Surg., 150: 7882, 1985.
- Christoforou M., Antonopoulos D., Danikas D. et al.:
Electrical burns in south-east Greece - Experience in the last three years, Ann. Medit.
Burns Club, 5: 31-2, 1992.
- Gordon M.W. G., Reid W.H. et al.: Electrical burns
incidence and prognosis in western Scotland. Burns, 12: 254-9, 1986.
- Lee R.C., Kolodney M.S.: Electrical injury mechanisms:
Dynamics of the thermal response. Plast. Reconstr. Surg., SO: 663-71, 1987.
- Lee R.C., Kolodney M.S.: Electrical injury mechanisms:
Electrical breakdown of cell membranes. Plast. Reconstr. Surg., 80: 672-9, t987.
- Govila A.: Early excision and primary resurfacing of wounds
following high voltage electrical burns. Eur. J. Plast. Surg., 12: 14754, 1989.
- Arturson G., fledlund A.: Primary treatment of 50 patients
with high tension electrical injuries. Scand. J. Plast. Surg., IS: 111-8, 1984.
| This paper was received on 21
September 1998. Address
correspondence to: Dr A.R.S El-Gallal
Head of Plastic and Burn Unit, AI-Jala Hospital, El-Arab Medical University
P.O. Box 795, Benghazi, Libya |
G. WHITAKER
INTERNATIONAL BURNS PRIZE
PALERMO, ITALY
Under the patronage of the Authorities of the Sicilian Region for 1998
By law n. 57 of June 14th 1983
the Sicilian Regional Assembly authorized the President of the Region to grant the
Giuseppe Whitaker Foundation, a non-profit-making organization under the patronage of the
Accadernia dei Lincei with seat in Palermo, an annual contribution for the establishment
of the G. Whitaker International Burns Prize aimed at recognizing the activity of the most
qualified experts from all countries in the field of burns pathology and treatment.
The amount of the prize is fixed at twenty million Italian Lire. The prize will be
awarded every year by the month of June in Palermo at the seat of the G. Whitaker
Foundation.
The Adjudicating Committee is composed of the President of the Foundation, the
President of the Sicilian Region, the Representative of the Accademia dei Lincei within
the G. Whitaker Foundation, the Dean of the Faculty of Medicine and Surgery of Palermo
University, the President of the Italian Society of Plastic Surgery, three experts in the
field of prevention, pathology, therapy and functional recovery of burns, the winner of
the prize awarded in the previous year, and a legal expert nominated in agreement with the
President of the Region as a guarantee of the respect for the scientific purpose which the
legislators intended to achieve when establishing the prize.
Anyone who considers himself/herself to be qualified to compete for the award may
send by January 3 1 st 1998 a detailed curriculum vitae to: Michele Masellis M.D.,
Secretary-Member of the Scientific Committee G. Whitaker Foundation, Via Dante 167, 90141
Palermo, Italy. |
|