| Annals of Burns and Fire Disasters - vol. XI - n. 4 - December 1998
TRACKING DYSPROTEINAEMIA IN THERMAL INJURIES
USING SERUM PROTEIN ELECTROPHORESIS
Wedler V., Prokop S., Künzi W., Meyer
V.E., Stocker R., Bürgî U.
Burns Centre, Clinic for Reconstructive Surgery,
University Hospital, Zurich, Switzerland
SUMMARY. Serum protein
electrophoresis is a routine method for diagnostics of dyslipoproteinaemia. The last 25
years' literature gives an extensive survey of the technical possibilities of separating
total plasma protein qualitatively and quantitatively in its fractions. Although there are
specific descriptions of dysproteinaemia for a multitude of acute and chronic diseases,
its course in thermal injuries has been little described. From February to October 1997
serum protein electrophoresis was performed prospectively in 24 patients suffering from
burn injuries, with total body surface ranging from 15 to 72% (mean: 30%). They were
followed from the acute phase until discharge from the intensive care unit. The individual
fractions were analysed and compared with each other. A typical curve with a compensatory
shift to the alpha-1 and alpha-2 fractions was demonstrated in serum protein
electrophoresis of the investigated burn patients. It is not sufficient to analyse only
total serum protein and alburnin concentration to control hepatic protein synthesis.
Analysis of the other protein fractions and different serum proteins (alpha-1 acid
glycoprotein, C-reactive-protein, high-density lipoproteins, low-density lipoproteins,
caeroluplasmin and transferrin) warrants consideration to prevent insufficient
substitution of alburnin with the possible risk of decreasing endogenous protein
synthesis.
Introduction
Serum protein electrophoresis is a routine
method used for diagnosing dysproteinaerma. The technical background to the qualitative
and quantitative separation of plasma proteins into individual fractions has been widely
covered in the literature of the last 25 years. Specific kinds of dysproteinaemia have
also been described for a large number of acute and chronic illnesses. Dysproteinaemia in
burn victims has, however, received only scant attention.
Between February and October 1997, we documented the results of serum protein
electrophoresis carried out on samples from 24 burn patients with TBSA between 15% and 72%
(average: 30%). Samples were taken throughout the patients' stay in intensive care.
In the phase immediately following a burn injury there is a well-known and characteristic
fall in total plasma protein, caused primarily by the massive loss of alburnin. Standard
clinical practice usually involves the subsequent measurement of total protein and
alburnin levels, both of which can remain depressed for days or even weeks despite
adequate patient nutrition. This research shows that in addition to this hypoalburninaemia
and hypoprealburninaemia, there is a reorientation of protein synthesis to favour the
alpha-I and alpha-2 fractions. Serum protein levels then normalize as treatment
progresses, with the exception of the gamma fraction, where depressed levels in the early
treatment phase are followed by a compensatory rise in the later stages. Serum protein
electrophoresis enabled us to identify these qualitative changes in protein synthesis in
burn victims, and made it possible to follow the typical development of these changes over
the course of treatment.
Serum protein electrophoresis is a routine method used for diagnosing dysproteinaemia.
Dysproteinaemia is a condition involving quantitative and qualitative changes in serum
proteins and is associated with a large number of disease conditions. Serum protein
electrophoresis is a tool used for identifying and monitoring changes in malignant
turnouts, indicators of acute and chronic inflammation, liver diseases, antibody
deficiencies, monoclonal gammopathies, etc. The heterogeneous mix of over 100 known serum
proteins can be separated into four component fractions (alpha-1, alpha-2, beta and gamma
globulins) (Table I) on a cellulose sheet in the electric field of the
electrophoresis chamber. At the same time, the relative proportion of the total protein
content represented by each individual protein can be calculated using the areas under the
individual peaks of the extinction curves.
Total protein 63-78 g/l
Fraction |
Absolute amount |
Relative amount |
Alburnin |
32.7 - 50.7 |
0.52 - 0.65 |
Alpha-1 globulins |
1.2 - 5.0 |
0.02 - 0.05 |
Alpha-2 globulins |
6.9 - 11.7 |
0.11 - 0.15 |
Beta globulins |
3.8 - 10.1 |
0.06 - 0.13 |
Gamma globulins |
6.3 - 1.8 |
0.10 - 0.19 |
|
| Table I - Serum protein and its fractions |
|
Given that the total protein content of
the relevant plasma is known, these relative values can be converted to absolute values.
Different authors have given different values for the concentrations of the individual
proteins in blood serum. The observations made in this research are compared with
reference values defined by our chemical institute (Table II).
Plasma protein
Fraction |
Function
Example |
| Alburnin |
Carrier, controlling colloid-osmotic pressure |
| Prealburnin |
Thyroxin-binding protein |
| Alpha-1 globulins Acid glycoprotein
Antitrypsin
Antichymotrypsin
High-density lipoproteins
Prothrombin
Transcortin
Foetoprotein |
Acute-phase-reaction (increase in cytolysis)
Inhibits trypsin, plasmin and elastase
Inhibits chymotrypsin
Lipid transport
Clotting factor II
Cortisol transport
Tumour marker (colonic and testicular carcinomas) |
| Alpha-2 globulins Cacruloplasmin
Antithrombin III
Haptoglobin
Macroglobulin
Pseudo CHE
Plasminogen |
Iron oxidation
Inhibits thrombin
Binds haemoglobin
Inhibits plasmin
Separate: acetyl - benzoyl - succinyl - butyrylcholine
Proenzyme |
| Beta globulins Low-density lipoproteins
Complement factor III
Haemopexin
Transferrin
Fibrinogen
CRP |
Lipid transport
Cytolysis: activating phospholipase
Protease
Binding haemin
Binding and transporting iron
Blood coagulation, inflammation reaction |
| Gamma globulins lgA
IgG
IgM
lgE
IgD
Lysozyme |
Antibody in body secretions
Unspecific cellular inflammation reaction
Early phase antibody
Antibody (allergic reactions)
Unspecific cellular inflammation reaction
Unspecific cellular inflammation reaction |
|
Table II
- Plasma proteins and their functions |
|
There is a dynamic balance between protein
biosynthesis, metabolization (especially in the peripheral organs), and excretion through
the gastrointestinal tract. All serum proteins are synthesized in the liver, with the
exception of the gamma globulins, which are produced in the beta lymphocytes. In a healthy
person, the alburnin-toglobulin ratio is 1.7 to 1.
Plasma proteins have the shortest half-life of all the proteins in the body and are
therefore particularly sensitive to acute or chronic changes in amino acid and protein
metabolism. The direct loss of these proteins through a traumatic event (such as acute
bleeding or open wounds) and/or relative loss through diffusion into extravasal space
(through leaking capillaries or following organ or multiorgan failure) can have a huge
impact on total protein content. Such losses result in the cessation or significant
impairment of particular functions performed by the proteins of one or all serum
fractions. Plasma proteins carry out a range of such functions: a nutritional function
(protein reservoir), a carrier function (they have large surface areas with numerous
hydrophilic and lipophilic bonding positions), maintenance of colloid-osmotic pressure
(through regulation of the distribution of water between plasma and interstitium), a
buffer function (constant pH), and protection from blood loss (fibrinogen).
Skin burns have major implications for alburnin loss since the skin stores between 30 and
40% of all alburnin in the body.
Materials and methods
The study was carried out between February
and November 1997, using 24 patients (19 men and 5 women) at the burns centre of the
Clinic for Reconstructive Surgery in Zurich University Hospital. The average TBSA of the
patients was 30% (range: 15-72%) and the average age of the patients was 40.4 yr (range:
20-88 yr). The average length of stay in intensive care was 23 days (range: 3-93 days).
Four of the patients died.
The patients all received surgical treatment which followed standard clinic practice: 1.
bath and debridement on arrival; 2. treatment of burns, using split-skin grafts after 34
days; 3. treatment of healing wound sites, using split-skin gra s or keratinocytes as soon
as the patient's clinical condition allowed. From arrival onwards, all patients received
enteral gavage feeding. A serum protein electrophoresis was carried out at regular
intervals of 1-2 days during the course of intensive care treatment, the latter being
categorized into acute, secondary, and post-secondary phases. Average absolute values were
calculated for each fraction and patient for each of these hospitalization phases. These
values were then used to calculate an average absolute value for each fraction across the
whole patient group. Absolute values were used when considering changes in protein levels
in individual patients, and relative values were used when comparing changes across the
group as a whole. Acid glycoprotein and high-density lipoproteins (HDL) (alpha- 1
fraction), caeruloplasmin (alpha-2 fraction), low-density lipoproteins (LDL), transferrin
and C reactive protein (CRP) (beta globulins) were also measured at the same intervals.
Further data regarding the group as a whole are given in Table III.
Patient
No. |
Sex
(m/f) |
Age
(yr) |
Burned area
TBSA % |
Intensive care
(days) |
| 1 |
m |
54 |
30 |
20 |
| 2 |
m |
42 |
32 |
13 |
| 3 |
m |
44 |
30 |
73 |
| 4 |
m |
38 |
51 |
51 |
| 5 |
m |
29 |
27 |
17 |
| 6 |
m |
23 |
31 |
14 |
| 7 |
m |
70 |
33 |
7* |
| 8 |
f |
24 |
40 |
13 |
| 9 |
f |
25 |
28 |
21 |
| 10 |
1 |
82 |
20 |
21 |
| 11 |
m |
34 |
34 |
17 |
| 12 |
m |
42 |
15 |
11 |
| 13 |
m |
30 |
22 |
14 |
| 14 |
m |
39 |
36 |
21 |
| 15 |
m |
49 |
15 |
13 |
| 16 |
m |
26 |
27 |
15 |
| 17 |
m |
31 |
38 |
33 |
| 18 |
f |
20 |
20 |
32 |
| 19 |
1 |
22 |
50 |
3 |
| 20 |
m |
88 |
45 |
7 |
| 21 |
m |
42 |
15 |
13 |
| 22 |
m |
48 |
65 |
93 |
| 23 |
m |
27 |
72 |
6* |
| 24 |
m |
33 |
27 |
24 |
| m/f = male/female; TBSA = total
burn surface area; * = deceased |
|
| Table III - The patients |
|
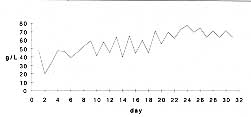
Results
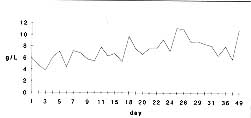
Total protein
All patients suffered from hypoproteinaemia during the first phase of treatment. In 17
patients this condition gradually disappeared. Fig. 1 illustrates this hypo- proteinaernia
during days 1-3 and the subsequent return to normal levels.
|
Fig. 1
- Total protein. |
|
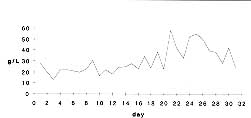
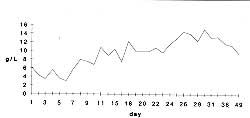
Alburnin and prealburnin
Absolute hypoalburninaemia and relative hypoalburninaernia were observed in all
patients at the beginning of treatment. Fig. 2 illustrates the deterioration in alburnin
levels between days 2 and 3 of treatment. Compared with the situation regarding total
protein, the return to normal levels began relatively late - from the second week of
treatment onwards. Prealburnin levels remained below normal (reference) levels throughout
the duration of the patients' stay in intensive care.
|
Fig. 2
- Alburnin. |
|
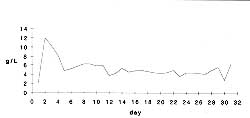
Alpha-1 fraction
In a compensatory reaction, the average value of the alpha-1 fraction rose steeply
during the first three days of treatment to well above normal levels. This value then
remained above the normal range, even though total protein levels were low, and returned
to normal (reference) levels only during the second phase of treatment (Fig. 3). With the
exception of one patient, HDL levels always remained within the reference range. Alpha
acid protein levels were higher than normal in all patients throughout their stay in
intensive care.
|
Fig. 3
- Alpha-1 fraction. |
|
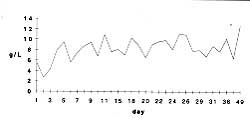
Alpha-2 fraction
From the third day of treatment, and despite the general hypoproteinaemia, alpha-2
fraction levels rose continuously and remained above normal values throughout treatment
(Fig. 4). Caeruloplasmin stayed at normal levels in all patients at all times.
|
Fig. 4 -
Alpha-2 fraction. |
|
Beta fraction
Although total protein levels were lower than normal, the beta fraction remained at
normal levels in 18 patients and was only slightly below normal throughout treatment in
six patients (Fig. 5). There were raised levels of CRP in all patients during the acute
treatment phase and at the beginning of the secondary treatment phase. LDL levels in 22
patients were below normal throughout treatment. Transferrin levels remained normal in 14
patients, but were lower than usual in 10 patients during the first two treatment phases.
|
Fig. 5
- Beta fraction. |
|
Alburnin substitution simply depresses the
body's own production of alburnin. Electrophoresis measurements, however, provide detailed
qualitative information about increases or decreases in the synthesis of proteins in each
individual fraction, information which can then be used more effectively in treatment or
the planning of diets.
Gamma fraction
Gamma fraction levels were below normal in the acute treatment phase and within the
reference range during the secondary treatment phase, rising above normal levels during
the final treatment phase (Fig. 6).
|
Fig, 6
- Gamma globulin |
|
Discussion
Changes in the constituents of the
individual protein fractions and changes in the relative amounts of each fraction in the
serum can be observed in many illnesses, and these changes are exploited in clinical
treatment. Pathophysiological regulatory mechanisms have yet to be fully investigated in
burn victims. The rapid development of dysproteinaernia at the beginning of the burn
trauma, as a consequence of alburnin loss, and nutrition-related dysproteinaemia during
treatment are well-known phenomena. The data from our patients showed that compensatory
changes took place in all serum protein fractions and we compared these with changes in
total protein levels. It was noticeable that the amount of alpha1 and alpha-2 proteins
rose, even though total protein levels were lower. This general hypoproteinaemia lasted
into the second week of treatment. There was also a delay before alburnin levels began to
return to normal. No alburnin substitutes were given to any patients. All protein
fractions fell below normal levels in days 1-3. Alpha-1 protein levels rose steeply in the
first two days of treatment (even though total protein levels were depressed). Levels then
returned to the upper reaches of the reference range from day 5 and remained constant
throughout the remainder of treatment, even though acid glycoprotein levels in all
patients were higher than normal throughout treatment. A compensatory rise in the alpha-2
fraction was observed from day 3 onwards and this continued throughout treatment, with
levels sometimes rising to as much as double normal values. Despite the increase in
c-reactive proteins in the first two thirds of treatment, b-fraction levels constantly
remained within the reference range. The gamma fraction rose parallel to total protein
levels and was at normal levels from the second treatment week onwards. After the third
week of treatment, gamma fraction levels rose above normal levels, despite
normoproteinaemia. We found that the results of serum protein electrophoresis in burn
victims describe a typical progression. During the acute phase, inflammation parameters
and proteins responsible for oxidative processes were at raised levels from day 2
posttrauma. An increase in acute phase proteins on days 6-8, as described by Moody, was
not observed.
Conclusion
We have to assume that the reorganization
of synthesis processes is achieved at the expense of some proteins. Increased LDL reflects
an increased demand for cholesterol (for production of steroid hormones and membranes and
as a key structural component of many tissue and plasma lipoproteins). If we are to
understand the various compensatory mechanisms taking place within each fraction in the
context of an overall hypoproteinaemia, then a range of known serum proteins will have to
be measured at regular intervals over the course of recovery from burn injuries. The
assumption currently made, i.e., that protein synthesis in the liver can be evaluated
through measurement of alburnin and total protein (and corrected by supplying alburnin
substitute), is not supported by this work. Alburnin substitution simply depresses the
body's own production of alburnin. Electrophoresis measurements, however, provide detailed
qualitative information about increases or decreases in the synthesis of proteins in each
individual fraction, information which can then be used more effectively in treatment or
in the planning of diets.
RESUME. L'électrophorèse
de la protéine sérique est une méthode de routine pour le diagnostic de la
dyslipoprotémémie. Depuis 25 ans la littérature présente toutes les possibilités
techniques pour séparer la protéine plasmatique qualitativement et quantitativement dans
ses fractions. Il y a des descriptions spécifiques de la dysprotéinémie relatives à
une grande varicté de maladies aiguës et chroniques, mais le cours de la dysprotéinemie
dans les brûlures a été rarement décrite. Dans la période février-octobre 1997 les
Auteurs ont effectué une étude de l'électrophorèse de la protéine sérique dans 24
patients atteints de brûlure, avec une surface corporelle totale brûlée entre 15 et 72%
(valeur moyenne: 30%). Les patients ont été étudiés depuis la phase aiguë jusqu'à la
sortie du service de réanimation. Les fractions individuelles ont été analysées et
confrontées entre elles. Une courbe typique avec un mouvement compensatoire vers les
fractions alpha-1 et alpha-2 a été démontrée dans l'électrophorèse de la protéine
sérique des patients brûlés étudiés. Il n'est pas suffisant d'analyser seulement la
concentration de protéine et d'alburnine du sérum total pour contrôler la synthèse de
la protéine hépatique. L'analyse des autres fractions protéiques (alpha-1
glycoprotéine acide, C-protéineréactive, les lipoprotéines à haute densité, la
céruléoplasmine et la transferrine) mérite d'être considerée pour prévenir une
substitution insuffisante de l'alburnine, avec le risque de diminuer la synthèse de la
protéine endogène.
BIBLIOGRAPHY
- Moody B.J., Shakespeare P.G., Batstone G.F.: The effects of
septic complications upon the serum protein changes associated with thermal injury. Ann.
Clin. Biochem., Jul. 22 (Pt 4): 391-6, 1985.
- Mullen J.L., Gertner M.H., Buzby G.P. et al.: Implications
of malnutrition in the surgical patient. Arch. Surg., 114: 121-5, 1979.
- Rhoads J.E., Alexander C.E.: Nutritional problems of
surgical patients. Ann. N. Y. Acad. Sci., 63: 268-70, 1955.
- Thomas L.: Serum-Eiweisselektrophorese. In: "Labor und
Diagnose", Die Medizinische Verlagsgesellschaft, Thomas L. (Hrsg), Marburg, 758-836,
1995.
- Sevaljevic L., Petrovic M., Savic J., Pantelic D.: The
effects of repeated thermal injury on rat liver and scrum protein synthesis rates. Comp.
Biochem. Physiol-13, 73: 379-84: 1982.
| This paper was received on 3 November
1998. Address correspondence to: Dr
Volker Wedler
Zentrum fur Brandverletzte, Klinik fur Wiederherstellungschirurgie
Universitdtspital, Ziirich, Ramistrasse 100, CH-8091 Zurich
tel.: 0041 1 255 1111; fax 0041 1 255 4563 |
|