Annals
of Burns and Fire Disasters - vol. XII - n. 1 - March 1999
THE EFFECT OF EARLY TUBE FEEDING ON SERUM
COPPER AND ZINC LEVEL IN BURNED CHILDREN
Gúmús N., Dalay C., Arsian E.,
Uslular S., Kivanc K.
Burn Unit of Plastic and
Reconstructive Surgery Department, Medical Faculty of Cukurova University, Adana, Turkey
SUMMARY. Copper (Cu) and
zinc (Zn) play an important role in biological and metabolic processes. These elements are
essential to man and have a beneficial effect on wound healing that is important in burn
patients. This study was designed to investigate the effect of early tube nutrition on
serum Zii and Cu levels after the administration of Zn- and Cu-containing nutrition
solutions. The study included 11 paediatric patients admitted within the first 30 h
post-burn. The burns were either deep partial- or full-thickness and the extent varied
from 12 to 35%. A commercial feeding solution containing 1 ing Cu and 12 mg Zn per 1 was
given at a rate of 10 ml/h via nasogastric or nasoenteral tube by a pump continuously at
the beginning and adding 10 ml per h. The daily caloric intake was calculated with the
Davies formula. Nutritional support was continued for 17 days post-burn. Samples of venous
blood were taken and analysed. A statistical comparison (Anova test) between the control
and therapy groups showed significant differences. The differences between the first
samples and the others were analysed by the Anova test but no significant difference was
observed. It was found that commercial nutritional solutions do not include sufficient
amounts of Zn and Cii to satisfy the requirements of paediatric patients. Supplementary
amounts must therefore be added.
Introduction
Copper (Cu) and zinc (Zn) play an
important role in biological and metabolic processes. These trace elements are essential
to man and have a beneficial effect on wound healing that is important in burn patients.
Cu and Zn are necessary for the functioning of a number of clinically important biological
enzymes, and the activity of these zinc-copper dependent enzymes is altered in particular
conditions of tissue destruction and repair. Deficiencies of one or more trace elements
can cause various diseases by affecting physiological and cellular functions. These
micronutrients may also affect the cardiovascular and immune systems.
Serum levels of Zit and Cu have been shown to be reduced after burn injury owing to
increased concentration in urine and exudate from the burn wound.` Some resuscitation
fluids, alburnin solutions, and blood and its products include Cu, Zn and other trace
elements. The use of these medications is ineffective to protect the serum and tissue
levels in burn patients. Total parenteral nutrition solutions contain trace amounts of
these elements but do not replace decreased trace elements in the serum of burn patients
without the addition of trace elements. Oral nutritional support may be preferred because
of the effect on the digestive system.
Oral nutrition can be administered after defecation in burned children in order to provide
clinical nutritional support. Feeding that is initiated within 48-72 h post-burn may be
defined as "early nutritional support' . A commercial nutrition solution containing a
greater amount of Cu. and Zn than other solutions was selected and a study was designed to
investigate the effect of early tube nutrition on the levels of serum Zit and Cu after the
administration of Zn- and Cu-supplemented nutrition solutions.
Materials and methods
This study included 11 paediatric
patients admitted within the first 30 h after burn injury to the Burn Unit at Plastic and
Reconstructive Surgery Department of the Medical Faculty at ~-'ukurova University in
Turkey. The study was performed between 1996 and 1997, with five male and six female
patients. The mean age was 5.9 yr (range, 2-15 yr). The burns ranged from 12 to 35% TBSA,
and were either deep partial or full thickness. The mean total burned surface area was
21.7%. There were five patients with flame burns and six with hot water scalds.
Patients were admitted in the first 4 to 30 h postburn (mean post-burn admission time, 14
h). Fluid resuscitation was started according to the Parkland formula. None of the
patients was given colloid solutions in the first 24 h. An enteral feeding tube (size 6 to
10 [French]) was inserted through the nares into the stomach or intestines and controlled
by x-ray film after admission. A commercial feeding solution containing 1 tug Cu and 12
ing Zn per 1 was given at a rate of 10 mil/h via nasogastric or nasoenteral tube by pump,
continuously at first and with 10 ml/h per h added. Nutritional support was continued for
17 days post-burn. Daily total caloric requirements were calculated with the Davies
formula (60 kcal/kg/day + 35 kcal/%/TBSA/day). The feeding solution contained 1 keal/ml
energy, 1 mg/1 Cu and 12 ing/1 Zir (Table I). The mean intakes of calories, Zii and
Cii in the 24 h post-burn were respectively 772 kcal, 9.27 Ing and 0.77 mg (Table H).
One, three, seven, ten, fourteen and seventeen days after admission samples of venous
blood were taken and analysed by flame atomic absorption spectrophotometry. Venous blood
samples from 40 healthy children were taken to check Zii and Cu serum levels. The Anova
test was used for the statistical analysis of the results (Table III).
| Osmolarity |
Calories (dl) |
Lipids |
Proteins (dl) |
Copper |
Zinc |
| 245 mosm/1 |
100 kea |
4.98 g |
3 g |
1 mgn /l |
12 mg/1 |
|
Table I - Content
of nutrition solution |
|
Patient
|
Age (yr) |
% TBSA |
Cu intake |
Zn intake |
Calorie intake |
| |
|
|
* |
** |
* |
** |
* |
** |
1 |
3 |
18 |
1.2 |
1.2 |
14.4 |
14.4 |
1200 |
1200 |
2 |
3 |
17 |
0.6 |
1.2 |
7.2 |
14.4 |
6000 |
1200 |
3 |
14 |
21 |
1.2 |
2.9 |
14.4 |
34.8 |
1200 |
2900 |
4 |
5 |
25 |
0.6 |
1.7 |
7.2 |
20.4 |
600 |
1700 |
5 |
15 |
21 |
0.65 |
2.4 |
7.8 |
28.8 |
650 |
2400 |
6 |
3 |
12 |
0.6 |
1.2 |
7.2 |
14.4 |
600 |
1200 |
7 |
5 |
25 |
0.6 |
1.7 |
7.2 |
20.4 |
600 |
1700 |
8 |
5 |
35 |
0.7 |
1.6 |
8.4 |
19.2 |
700 |
1600 |
9 |
5 |
28 |
0.81 |
3.5 |
9.72 |
42 |
810 |
3500 |
10 |
2 |
17 |
0.95 |
1.7 |
11.4 |
20.4 |
950 |
1700 |
11 |
5 |
20 |
0.59 |
1.8 |
7.08 |
21.6 |
590 |
1800 |
| Mean |
5.9 |
21.7 |
0.77 |
1.9 |
9.27 |
22.8 |
77 |
1900 |
*
Intake in first 24 h post-burn
** Daily intake 24 h post-burn |
|
Table II - Daily
caloric intake, Cu and Zn |
|
Post-burn
days |
Serum
level of Cu
(mean + SD) µg/dl |
Serum
level of Zn
(mean + So) µg/dl |
1 |
80.83 ± 11.04
|
72.91 ± 15.73
|
3 |
80.90 ± 19.97
|
70.45 + 17.18 |
7 |
85.00 ± 19.62
|
72.27 ± 14.38
|
10 |
86.36 + 14.84 |
65.00 + 11.83 |
14 |
84.37 + 15.45 |
64.37 ± 10.15
|
17 |
76.66 ± 9.83 |
64.16 + 13.93 |
Control (n =
42) |
99.12 ± 10.91
|
86.25 ± 12.94
|
|
Table III- Serum
copper and zinc levels |
|
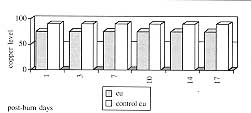
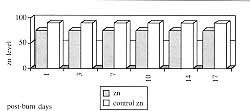
In this study, serum Cu and Zn levels
were determined on six occasions in 11 children. Within 24 It of injury, a mean dose of Zn
and Cu (9.27 and 0.77 mg, respectively) was being administered continuously via tube
feeding by means of a nutrition pump (range for Zn, 7.08 to 14.4; for Cu, 0.59 to 1.2). On
the following days the mean copper and zinc intakes were respectively 1.9 (range, 1.2-3.5)
and 22.8 (range 14.4-42.0) mg. No patient received additional Cu or Zn supplementation
during the study period of 17 days in response to serum Zn or Cu results. The mean Cu and
Zn levels were found to be 99.12 ± 10.91 and 86.25 ± 12.94 pg/dl in the control group
(Figs. 1, 2). A statistical comparison between control and the therapy group on different
days showed a significant difference (p > 0.05). When the differences between the first
samples and the others were analysed, no significant differences were observed (p <
0.05).
|
|
| Fig.
1 - Change of serum copper level on different days. |
Fig.
2 - Change of serum zinc level on diferent days. |
|
Discussion
The choice of type of nutrition type
depends on each patient's individual needs, physical characteristics, and the type and
duration of the burn injury. In seriously burned patients, there is a tendency towards
hypercatabolism, especially if nutrition is not initiated within the first 24 h post-burn.
The administration of nutritional substrates in the first few days postburn protects the
digestive system, counteracts infection, and prevents malnutrition by slowing down
hypercatabolism.` If enteral nutrition is carefully planned and properly managed, the
typical septic complications of parenteral nutrition therapy do not occur. Post-burn
hypozincaemia and hypocupraemia have been well described. Although serum Zn and Cit
concentrations tend to fall, urine excretion increases and minerals are thus lost from the
body.
Berger et al.'studied the influence of large intakes of trace elements on serum levels in
major burns. They showed that after daily administration of 4.5 ing Cri and 40.0 mg Zn, Cu
and Zit status were improved in adult burn patients. In our study, the administration of 1
mg Cit and 22.8 mg Zn did not improve serum levels compared with control values. Both Zn
and Cu decreased in all the samples. This lower serum level may be related to differences
in metabolism or other requirements in children. The different results may be related to
the administration of lower dosages. Bottschlich and Warden recommended 100 ing zinc daily
for burned children under 3 years of age and 220 ing daily for those aged over 3 years.
Gosling et al.' observed that although the mean daily Cu and Zn intakes were respectively
4.2 and 19.7 ing (respective ranges, 1.7 to 10.8 and 9 to 39), hypocupraemia and
hypozincaemia were found. Serum copper concentration was inversely correlated with the
burn surface area and hypozincaemia was found in adult patients irrespective of the burn
surface area. During our study, despite the fact that mean quantities of 1.9 ing Cu and
22.8 mg Zn were administered 24 h post burn, and nutritional support - including trace
elements - was initiated in the first 24 h post-burn period, hypozincaemia and
hypocupraemia were nevertheless observed.
In this study, it was observed that commercial nutritional solutions do not include
sufficient amounts of Zn and Cit to satisfy the requirements of paediatric patients.
Supplementary quantities of these elements have to be added. Paediatric burn patients need
to be supported with greater amounts of trace elements than patients with other injuries.
Further research is required to establish the quantities required for the restoration of
decreased Zn and Cit serum levels.
RESUME. Le cuivre (Cu) et le
zinc (Zn) jouent un rôle important dans les processus biologique et métabolique. Ces
éléments sont essentiels pour l'homme et ils exercent un important effect positif sur la
guérison des lésions des patients brűlés. Cette étude a considéré l'effet de la
nutrition précoce nasogastrique et nasoentérale sur les niveaux sériques de Zn et de Cu
aprčs l'administration de Zn et de Cu qui contenaient des solutions nutritives. L'étude
comprenait 11 patients pédiatriques hospitalisés dans les premičres 30 aprčs la
brűlure. Nous avons administré une solution nutritive commerciale contenant 1 mg Cu et
12 mg Zn par litre dans la mesure de 10 ml/h moyennant tube nasogastrique ou tube
nasoentéral avec l'emploi d'une pompe, continűment d'abord et augmenté dans la mesure
de 10 ml/h par heure. L'apport journalier de calories a été calculé avec la formule de
Davies. Le support nutritif continuait pour 17 jours aprčs la brűlure. Des
prélčvements de sang veineux ont été analysés et une recherche statistique (test
Anova) entre les témoins et le groupe traité a démontré des différences
significatives. Les différences entre les premiers prélčvements et les autres ont été
analysées moyennant le test Anova sans trouver aucune différence significative. Les
Auteurs ont observé que les solutions nutritives commerciales ne contiennent pas une
quantité suffisante de Zn et de Cu pour satisfaire les besoins alimentaires des patients
pédiatriques. Pour cette raison il faut que ces éléments soient administrés en
quantité adéquate.
BIBLIOGRAPHY
- John H., Marion S.: Zinc concentrations within healing
wounds. Arch. Surg., 100: 349-57, 1970.
- Selmanpakoglu A. N., (~etin C., Sayal A.: Trace element
(AI, Se, Zn, Cu) levels in serum, urine and tissues of burn patients. Burns, 20: 99-103,
1994.
- Gosling P., Rothe H.M.: Serum copper and zinc concentration
in patients with burns in relation to burn surface area. J. Burn Care Rehabil., 16: 481-6,
1995.
- Berger M.M., Cavadini C.: Unrecognised intake of trace
elements in polytraumatized and burned patients. Ann. Fr. Anesth. Reanim., 13: 289-96,
1994.
- Raff T., Hartman B.: Early intragastric feeding of
seriously burned and long-term ventilated patients: a review of 55 patients. Burns, 23:
19-25, 1997.
- Rodriguez D.J.: Nutrition in patients with severe burns:
state of the art. J. Burn Care Rehabil., 17: 62-70, 1996.
- Cucchiara P_ Masellis M_ Sucameli M.: Considerations on
nutritional therapy in the burn patient. Ann. Burns and Fire Disasters, 9: 30-2, 1996.
- Holland K.A., Gillespie R.W.: Estimating energy needs of
pediatric patients with burns. J. Burn Care Rehabil., 16: 458-60, 1995.
- Berger M.M., Cavadini C.: Influence of large intakes of
trace elements on recovery after major burns. Nutritious, 10: 327-34, 1994.
- Moylan J.A..: Burn injury. In: "Textbook of Plastic,
Maxillofacial and Reconstructive Surgery", Gregory S.G., Nicholas G.G. (eds), 2nd
ed., Williams and Wilkins, Baltimore, p. 243, 1992.
| This paper was received on 28 July 1998. Address correspondence to: Dr Nazim Gumus
Qukurova Universitesi Tip Fakultesi Plastik ve Rekonstruktif Cerrahi Anabilimdali
Balcali
Adana, Turkey
tel.: 090 338 6060 / 3226; fax: 090 338 6427 |
|