Annals
of Burns and Fire Disasters - vol. XII - n. 1 - March 1999
TISSUE EXPANSION: A POSSIBLY VALID
RECONSTRUCTIVE ALTERNATIVE IN ELECTRIC BURNS OF THE MOUTH
Atiyeh B.S.
Division of Plastic and
Reconstructive Surgery, American University of Beirut Medical Centre, Beirut, Lebanon
RESUME. Electric burns in
general are relatively rare. In electric burn accidents, particularly in adults, hand
injuries prevail. in children, however, the most common electric injuries are burns of the
mouth, with 90% of such burns occurring in infants and toddlers less than four years of
age. These burns are among the saddest, most devastating, and most difficult types of
injury to correct. There is great confusion in the literature about the proper management
of electric burns of the mouth in the acute phase. There is even greater confusion when it
comes to secondary correction of the resultant deformity. Nearly all the surgical
reconstructive techniques that have been described result in serious mutilation of the
surrounding normal tissues and fail to simulate a normal oral sphincter. An attempt was
made to expand remaining normal lip tissues in a child by simulating a technique that has
been performed for many ages by populations throughout Africa, America, and the South
Pacific. The expansion device has yet to be perfected, but in principle the idea is
appealing since the condition of microstornia secondary to electric burns of the mouth can
be corrected by expanding residual normal lip segments.
Introduction
Electric burns in general are
relatively rare. They account for only 4 to 7% of admissions to major burn centres.`21n
electric burn accidents, hand injuries prevail, particularly in adults.'ln children,
however, burns of the mouth are the most common electric injuries,'with 90 % of burns
occurring in infants and toddlers under four years of age, with a preponderance of boys.
1,4,5 Such burns can be among the saddest, most devastating, and most difficult types of
injury to correct.'
Mechanism of injury
Most electric mouth burns are
secondary to domestic accidents and are caused by low-voltage low-frequency alternating
current in the range of 110 to 220 V and 5060 ke. Although frequently considered to be
harmless, 110 V circuits can be fatal when the current passes through the chest secondary
to extensive contact and good grounding. Most electric mouth burns, however, have their
entry and exit points localized in the perioral area, and fatal accidents are unusual.
In the majority of patients the injury occurs when the child sucks or bites the free end
of a "live" extension cord. The current flows from the hot lead to the neutral
lead through the path of least resistance. When distant resistance is high, the current
flows only through the adjacent tissues. If distant resistance is low and the patient is
well grounded, the current passes through the body across the chest to the point of exit.
The resistance of dry skin is high, ranging between 40,000 and 100,000 ohms per square cm.
Wet skin has a resistance of 1200 to 1500 ohms per square em, while the resistance of
mucous membranes is as low as 100 ohms per square cm.
Tissue injury in an electric burn of the mouth depends on the voltage, duration of
contact, tissue resistance, type of current, and the path the current takes from entry to
exit. The resultant wound is a combination of are burn and contact burn. When
electrolyte-rich saliva bridges the gap between two wires of opposing polarity, an arc is
produced releasing flash heat in the order of 2500 to 3000 °C. A contact burn occurs when
the electric current effectively passes through tissue planes to the point of exit,
generating heat along its pathway. Household alternating current produces more local
tissue damage than direct current of the same voltage and can produce tetanic muscle
contraction which prolongs the duration of contact.
Pathophysiology
Initially, demarcated electric burns
of the mouth are painless and appear as necrotic grey wounds with a surrounding rim of
erythema. Within 4-6 h there is increasing oedema. If such injuries are seen within the
first 12 h, some authors believe that there is an easily identifiable definite line of
demarcation present between healthy and burned tissues which allows immediate surgical
debridement. However, most surgeons experience some difficulty in forming an accurate
determination of the injury zone before separation of the necrotic eschar at around 14
days. Progressive tissue necrosis secondary to small vein thrombosis is uncommon but major
bleeding from the coronary labial artery can occur as late as two weeks post burn? The
concept of progressive creeping necrosis in electric burns has been lately challenged.
Apparently, what is termed creeping necrosis is in fact inadequate initial determination
of tissue destruction.
The lower lip and oral commissures are most commonly involved in electric burns.Along with
the oral soft tissues, the teeth and supporting periodontiurn may be injured with
resultant cross bite, crowding and deviation of the dentition, and varying degrees of
malocclusion. Growth of the anterior alveolar process also may be affected. Associated
burn of the tongue, even when extensive, heals spontaneously and has never been reported
to disturb speech.
After separation of the eschar, secondary wound healing proceeds, resulting in severe
scarring particularly if the burn has been complicated by infection, microstomia, and
drooling due to obliteration of the buccal sulcus.
Case presentation
A three-year old child recently
presented to the American University of Beirut Medical Centre with electric burn of the
mouth. The injury occurred when the child bit the male plug of a live extension cord
connected to a private generator, an injury mechanism common to the majority of electric
burns among children in Lebanon. The injury involved more than two-thirds of the lower lip
as well as the tip of the tongue and parts of the upper lip and left oral commissure. The
child was managed conservatively with frequent cleansing and topical antibiotic ointments
until secondary healing was complete. He was then fitted with a dynamic splint constructed
by a dental prosthodontist, which was worn for six months until the scars matured. The
splint prevented the formation of severe microstomia and at the same time expanded the
remaining normal lower lip segments. Secondary corrective surgery was specifically
restricted to excision of the scar and primary approximation of the remaining lower lip
lateral segments with a limited left commissuroplasty. Expansion of the lower lip was
resumed post- operatively, using initially the same dynamic splint and subsequently an
intraoral device, the anteroposterior projection of which was gradually increased (Fig.
1). Satisfactory lower lip reconstruction was achieved with limited surgery, totally
avoiding mutilation of surrounding normal tissues (Figs. 2, 3).

|
 |
 |
 |
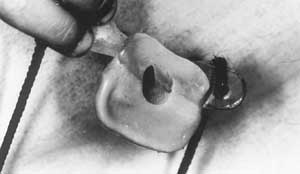
Fig. 1 -
The constructed expander. The anteroposterior dimension is gradually increased by
overlaying dental wax. |
Fig. 2 -
(above) Lower lip appearance after simple scar excision and limited commissuroplasty;
(below) Lower lip expanded. The same apparatus is used to deepen the labial sulcus. |
|

|

|
Fig.
3 - Profile view of lower lip without and with expander in position. |
|
Discussion
There is great confusion in the
literature regarding the proper management of electric burns of the mouth. Owing to the
rarily of' the condition, most of the series that have been reported are relatively
limited in number. They all reflect personal experiences and impressions gained over an
extended period of time rather than the results of a scientifically conducted double-blind
prospective study comparing the results of various treatment protocols. Among the largest
series reported are that of FoghAnderson and Sorensen' in 1966 regarding 68 children,
representing their experience in Denmark over 30 years, and that of Thomson et All. in
1965, regarding 45 cases treated at the Hospital for Sick Children in Toronto over an
18-year period.
The majority of authors advocate conservative treatment for electric burns, allowing
spontaneous healing to occur, followed at a later stage by reconstructive procedures,'
because of the difficulty of assessing the degree of initial injury and in order to
minimize the loss of valuable normal tissue during early excision. It is surprising to
find that even moderate primary defects can heal and leave very slight secondary
deformity, if any at all. When reconstructive surgery is required secondarily, repeated
minimal local procedures that avoid the use of major flaps have been found to be most
gratifying, minimizing the risk of additional new scars and disfigurement. No specific
operation is advocated for routine use. The surgical procedure is selected on an
individualized basis depending on the soft tissue defect.
Conversely, other surgeons have found that it is theoretically unwise and aesthetically
displeasing to allow the injuries offiatients with severe electric burns of the mounth to
heal spontaneously because the mouth plays a critical role in the aestethic balance and
unity of the face, apart from its equally important function. Clinically, the demarcation
line is quite obvious 14 days post-injury. It is therefore advisahlc to delay surgical
debridement and reconstructive surgery until then. Wailing any longer to correct the
deformity may not be advantageous to the patient.
Others recommend early debridernent and reconstruction. Hyslop maintains that if electric
burn of the mounth are seen and treated within the first 12H post burn, there is a
definite line of demarcation that allows immediate surgical tretament, shortens healing
time, and minimized the number of reconstructive procedures. Secondary infection can he
avoided if surgery is performed no later than 4 to 7 days post-injury.
Thomson et al. found that there was no signilicant difference in morbidity or cosmetic
results between patient, operated on before the burn had healed and those in whom
operative procedures were delayed until complete healing.
The introduction of mouth splints was an important addition to the management of electric
burns of the mounth. Again there is no agreement in the literature as to the type of
splint to be used or when it should be applied. The problems associated with the use of
oral splints for the treatment of electric burns of the mouth have been twofold. The first
problem relates to the mechanical retention of particularly since the patients affected
are toddlers who do not have all the primary teeth or are in a phase of active dental
eruption. The second problem is the psychological acceptance of the splint by the child
and its parents. Wearing a splint after a burn helps to prevent secondary contractures and
leads to faster maturation of flow thus allowing earlier secondary corrective surgery.
Satisfactory results were achieved when the splint was applied early, before complete
wound healing, especially when the oral commissure was involved, although significant
bleeding occurred in about 7% of the cases Placement of the splint within 10 to 14 days of
the injury, after the eschar has sloughed, allows approximahon ol proper lip dimensions.
The appliance is worn 24H a day for the first six months and 12H a day for six more
months. With this regimen, the majority of electric burns of the mouth do not require
secondary corrective surgery but, when they do, the required procedure is usually minor
and successful in creating a natural appearance. Although longterm wearing of the splint
is required, most children apparently tolerate it well.
The expansion of various facial structures is not in the history of humanity. In many
African tribes, the ears are perforated in childhood and gradually stretched to hum great
loops serving a decorative purpose. Wooden plugs of increasing size are used to stretch
the loop. A similar practice on the nose is ubiquitous among primitive New Guincans.
Stretching the lips is also popular in Brazil as well as in Africa. In Africa, this forin
of mutilation was probably begun centuries ago to make women unattractive to slave
traders. In the years that followed, the fashion caught on, and such women came to be
considered appealing. Ironically, this mutilating practice can now be adapted and used to
advantage for lip expansion in a child mutilated by electric burn. Technically this is not
easy to perform, but it should not pose insurmountable problems. In the case we present,
both child and family showed good toleration of the whole lengthy process.
Conclusion
The management of electric burns of
the mouth is a long and laborious endeavour. Patience is required from both the treating
physician and the child's family. Irrespective of the method of treatment, the goal should
always be restoration of normal aesthetic and functional anatomy, with the least amount of
scarring. Unfortunately, until now, plastic surgery has not found a way to reconstruct
normal dynamic sphincters, which are what the lips are. Lip expansion could be a new,
beneficial, reconstructive method. The expansion device still needs to be perfected, but
the idea is appealing in principle since the resultant microstomia following electric burn
of the mouth can be corrected by expanding residual normal lip segments. Prevention of
electric burns of the mouth remains the best policy. Live extension cords are a definite
hazard for young children in the home. Prophylactic steps should be taken to prevent the
occurrence of such catastrophes.
RESUME. En général les
brûlures électriques sont relativement rares. Dans la plupart des brûlures provoquées
accidentellement, il y a une prédominance des lésions de la main, particulièrement dans
les adultes, tandis que dans les enfants les brûlures de la bouche sont les plus communes
et constituent 90% des brûlures qui intéressent les enfants âgés moins de 4 ans. Ce
type de brûlure est un des plus dévastants et angoissants et très difficile à traiter.
Dans la littérature règne une grande confusion pour ce qui concerne la gestion correcte
des brûlures électriques de la bouche dans la phase aiguë, mais la confusion pour ce
qui concerne la correction secondaire des défauts qu'elles causent est encore plus
grande. Presque toutes les techniques reconstructrices chirurgicales décrites dans la
littérature provoquent une grave mutilation des tissus normaux adjacents et ne
réussissent pas à simuler le sphincter oral normal. L'Auteur a effectué une épreuve
pour augmenter les tissus résiduels des lèvres dans un enfant, en simulant une technique
employée depuis des siècles innombrables par des tribus en Afrique, en Amérique et dans
le Pacifique Méridional. L'appareil utilisé pour l'expansion des tissus doit encore
être perfectionné mais le principe de base est intéressant, puisqu'il offre la
possibilité de corriger la microstomie secondaire aux brûlures électriques de la bouche
moyennant la technique de l'expansion des segments normaux résiduels des lèvres.
BIBLIOGRAPHY
- Fogh-Andersen P., Sorensen B.: Electric mouth burns in
children: treatment and prevention. Acta Chit. Scand., 131: 214, 1966.
- Skoog T.: The surgical treatment of burns. Acta Chit.
Scand., Suppl. 305:115,1963.
- Dado D.V., Polley W., Kernhan, D.A: Splinting of oral
commissure electrical burns in children. J. Pediatr., 107: 92, 1985.
- Thomson H.G., Juckes AW., Farmer AW.: Electric burns of the
mouth in children. Plast. Reconstr. Surg., 35: 466, 1965.
- Port R.M., Cooley R.O.: Treatment of electrical burns of
the oral and perioral tissues in children. Am. Dent. Assoc., 112: 352, 1986.
- Brown J.B., Fryer M.P.: Reconstruction of electric
injuries, including cranial losses. Ann. Surg., 146: 342, 1957.
- Fogh-Andersen P., Sorensen B.: Electric oral burns in
Danish children with special reference to prevention. Scand. J. Plast. Surg., 18: 107,
1984.
- Hyslop V.B.: Treatment of electric burns of the lips.
Plast. Reconstr. Surg., 20: 315, 1957.
- Chick L.R., Lister G.D., Sowder L.: Early free-flap
coverage of electrical and thermal burns. Plast. Reconstr. Surg., 89: 1013, 1992. 10.
Ortiz-Monasterio F., Factor R.: Early definitive treatment of electric burns of the mouth.
Plast. Reconstr. Surg., 65: 169, 1980.
- Kazanjian V.H., Roopenian A.: The treatment of lip
deformities resulting from electric burns. Am. J. Surg., 88: 84, 1954.
- Wells D.B.: The treatment of electric burns by immediate
resection and skin graft. Ann. Surg.: 90: 1069, 1929.
- Fleurey A.F.: Electrical burns of the lips: a modified plan
of treatment. Am. Surgeon, 25: 328, 1959.
- Colcleugh R.G., Ryan J.E.: Splinting electric burns of the
mouth in children. Plast. Reconstr. Surg., 38: 239, 1976.
- Rees T.D.: Concepts of beauty. In: "Aesthetic Plastic
Surgery", Thomas D. Rees (ed.), W.B. Saunders Co., Philadelphia, vol. 1: 115, 1980.
| This paper was received on 10 December
1998. Address correspondence to:
Dr Bishara S. Atiyeh, Division of Plastic and Reconstructive Surgery,
American University of Beirut Medical Centre, Beirut, Lebanon,
or c/o American University of Beirut New York Office,
850 Third Ave., l8th Floor, New York, NY 10022
(fax: 961 1 744464).. |
|