Annals
of Burns and Fire Disasters - vol. XII - n. 1 - March 1999
RECONSTRUCTION OF VULVA IN A FEMALE
PATIENT HAVING LONGSTANDING GENITAL BURN CONTRACTURE WITH SEVERE WEB AND MARJOLIN'S ULCER:
A CASE REPORT
Sonmez Ergun S, lscen Cek D, Ulay
M.
Department of Plastic and
Reconstructive Surgery, Vakif Gurepa Hospital, Istanbul, Turkey
SUMMARY. In
this report, a 17-year-old female patient with a post-burn genital contracture that caused
severe deformity and squarnous cell carcinoma and the results of the genital web release
and vulva reconstruction with our flap design are presented.
Introduction
Burn injuries involving the genital
area are rarely seen owing to the anatomical features of the region. The elasticity and
laxity of the skin in this region are very important. The characteristics of the skin
after thermal injury may be lost so that extensive contractures may occur. The diagnosis
and treatment of this type of burn sequela are frequently delayed owing to the patients'
ignorance or shyness. This delay can be extended until puberty and sometimes even later in
females.
Case report
A 17-year-old white was female
admitted to our department with an ulcerovegetant tumoral mass on the superornedial side
of the left thigh. She had undergone thermal burn injury ten years previously. The wounds
were treated conservatively, but severe scars, involving the pubic area, both inguinal and
in the upper thigh anteriorly and posteriorly, developed. The web in the inguinal area
caused walking, sitting, urination and defecation difficulties. The ulcerovegetant tumoral
mass on the superomedial side of the left thigh was 12 x 12 cut in size with progressive
enlargement in the last 8 months. A soft, mobile, painless lymph node 0.5 x 0.5 cm in size
was palpated in the ipsilateral inguinal area. Systemic examination revealed no additional
pathology (Fig. 1).
Ablation of the tumoral mass, nodal biopsy, and web release with skin grafting were
planned.

|

|
Fig. la
- Pre-operative anterior view. |
Fig. 1b -
Pre-operative posterior view. |
 |
Fig. lc -
Pre-operative lateral view. |
|
Surgical technique
The tumoral mass was excised with a 2
cm intact margin and the node was extirpated. The histopathological examination revealed
that the tumoral mass was a welldifferentiated squarrious cell carcinoma; the surgical
margins were reported to be turnour-free. The diagnosis of the nodal biopsy was reactive
hyperplasia.
Incising bilaterally, 2 cm caudal and parallel to both inguinal creases and joining at the
inferior border of the web, two flaps were formed. The genital web was released in such a
manner that the tissue forming the abdominal side of the web was utilized for pubic
reconstruction as a flap with superior pediele, while the perineal side was used for the
upper part of the vulvar reconstruction in Zplasty fashion (Fig. 2).
|
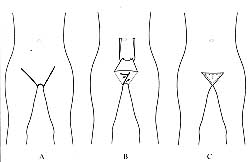
Fig. 2
- Drawings of the procedure. A) Anterior side of flap design. B) Planning of Z-plasty on
posterior side after elevation of flap. Q Final shape of pubic area after operation. |
|
The secondary defects after
turnoral mass excision and the release in both the inguinal and the upper thigh area were
reconstructed by STSG harvested from the posterolateral thigh (Figs. 3, 4). The
patient did well post-operatively. In the follow-up period, no recurrence or metastasis
was found up to two years postoperatively.
Discussion
Burn injuries involving the genital
area are seen rarely, probably due to the anatomically hidden location. These injuries may
occur as part of the extensive burns of the lower trunk and thighs. In secondary healed
cases, severe contractures and bridges may occur.
Since the contracture is not in a stabilized position, recurrent ulcerations may occur,
and in exceptional cases Marjolin's ulcer may develop, as in our patient. Treatment of
Marjolin's ulcer is entirely surgical, sometimes with a combination of radiotherapy and
chemotherapy according to the stage of the tumour. Surgical treatment is wide monoblock
resection.
The overall incidence of regional lymph node metastases in the trunk and extremities
appears to be 25%, but the controversy regarding prophylactic nodal dissection still
exists. Further information is needed to establish the validity of predictive factors such
as size and depth of invasion.
Clinically enlarged regional lymph nodes were subjected to biopsy and patients with
biopsy-proved nodal metastases were treated by nodal dissection radiation and chemotherapy
if necessary. Proper initial treatment of burns, with early use of skin grafts, might
prevent the development of these potentially serious tumours.
In conservatively treated cases, many of the problems - severe contractures and web
formation causing difficulties with walking, sitting, urination and defecation - may be
encountered as a result of the natural trend of thigh adduction. The abnormal appearance
and the contracture may prevent the patients having a normal sexual life, with consequent
psychological problems. Thus, in the management of burn sequelae of the area and
especially in vulvar reconstruction, not only the functional aspect but also the cosmetic
appearance should be primary aims. Reconstruction should be performed in harmony with
anatomical factors.
Various surgical procedures have been suggested and utilized for the release and
reconstruction of post-burn webs in the genital area. These range from simple release and
skin grafting to a number of different flap procedures, including Z-plasty, V-Y plasty,
5-flap plasty, doubleopposing Z-plasty, and other local flap uses. Tissue expansion can be
utilized.
In our patient, after release of the web with the flap elevated anteriorly, the pubic area
presented an almost normal anatomical appearance. Also, tailoring of the posterior side of
the genital web in Z-plasty fashion relieved the retraction involving upper parts of the
labia majora, resulting in the vulva having a normal anatomical appearance.
This method minimizes the necessity of grafting. A natural appearance of the pubic and
vulvar areas was obtained that cannot be observed with other procedures.
We conclude that a highly acceptable functional and aesthetic result was achieved by our
flap design.
RESUME. Les Auteurs
présentent le cas d'une patiente de 17 ans atteinte d'une contracture génitale due à
des brûlures qui a causé une déformation sévère et un carcinome épidermoide. Les
résultats, de la reconstruction de la vulve effectuée moyennant notre système sont
présentés, avec une revue de la littérature en rapport.
BIBLIOGRAPHY
- Alghanem A.A., McCauley R.L., Robson M.C., Rutan R.L.,
Herndon D.N.: Management of pediatric perineal and genital burns: twentyyear review. J.
Burn Care Rehabil., 11: 308, 1990.
- Joucdar S., Kismoune H., Boudjemia F., Bacha D., Abchiche
M.: S&quelles de br6lures abdomino-p6rin6ales - ~ propos de trente cas. Ann. Medit.
Burns Club., 8: 103, 1995.
- Luce E.A.: Oncologic considerations in nonmelanotic skin
cancer. Clin. Plast. Surg., 22: 39, 1995.
- Broadland D.G., Zitelli J.A.: Surgical margins for excision
of primary cutaneous squamous cell carcinoma. J. Am. Acad. Dermatol., 27: 108, 1992.
- Shin M.H., Chu F., Fortner J.G.: Treatment of regionally
advanced epidermoid carcinoma of the extremity and trunk. Surg. Gynecol. Obstet., 150:
558, 1980.
- Bangma C.V., van der Molen A.B.M., Boxma H.: Burns to the
perineal and genitals - management, results and 'function of the thermally injured
perineum in a 5-year review. Ent. J. Plast. Surg., 18: 111, 1995.
- Cek C.I., Ergun S.S., Cek M., Akbay S., Guneren E.: Genital
ve bolge yaniklari. Turk. Plast. Rekonstr. Cerrahi Derg., 4: 159, 1996.
- Muir I.F.K., Morgan B.D.G.: Burns of genitalia and
perineum. "Plastic and Reconstructive Surgery of the Genital Area", Horton C.G.,
Little Brown G., 447, 1993.
This paper was received on 26 September 1998.
It was presented at the Nineteenth National Congress of
Turkish Society of Plastic Surgeons held
in Antalya, Turkey, in September 1997.Address correspondence to: Dr
Selma Sonmez Ergun
Bahceseir Emlak Konutlan, BIS D3 C020403, 34900
Buyukcekmece, Istanbul, Turkey
tel.: 90 212 669 0835; fax: 90 212 240 5904 |
|



