Annals of
Burns and Fire Disasters - vol. XII - n° 2 - June 1999
USE OF MEPITEL* ON GRAFTED AREAS IN BURN PATIENTS
Deved M, Sengezer M, Kopal C.
Department of Plastic and Reconstructive Surgery and Burn Centre, Gülhane Military
Medical Academy, Turkey
SUMMARY.
Autografting is the best procedure for replacing skin defect due to deep dermal burn.
Currently, textile dressings are frequently preferred for grafts. This dressing material
does not however fix the graft sufficiently well and may damage the graft, also causing
maceration and pain in the graft area during dressing changes. In this study, a
silicone-coated polyamide dressing material was used for graft dressing and its effects on
graft take rate were investigated. Silicone-coated polyamide (Mepitel/SCA Molnlycke) is an
elastic transparent, non-adherent, porous material. Mepitel's porous structure permits
wound exudate to pass directly into absorbent dressings. Mepitel adheres to dry skin but
not to moist wounds. In this study, conducted between May 1997 and May 1998, eighteen
patients (mean age, 23 yr; mean total body surface area burned, 12%) were treated at the
GUlhane Military Medical Academy Burn Centre in Turkey. All the patients had Mepitel
dressings applied over their grafts. Suction compresses were changed on post-operative day
4 without Mepitel being removed. The compresses were changed until post-operative day
8-12, but not Mepitel. The grafts were easy to observe because of Mepitel's transparence,
and exudate was evacuated by its porous structure. Graft take was above 90% in all cases.
Minimal graft loss was observed in patients receiving Mepitel as a graft dressing. In
conclusion, Mepitel was found to be effective for graft take and facilitated the
observation of haernatorna and serorna.
Introduction
The ideal skin replacement after thermal
injury to the skin is autograft, i.e., integration of the epidermis by means of a basement
membrane zone to the dennis. Functionally, the epidermis controls evaporative losses and
provides immunological protection, while the dermis serves principally for early
tangential excision, and the autograft technique is reported to be the mainstay in the
management of deep burns.
Although thermal injury mainly affects the skin, mortality and morbidity are still
important owing to postburn immunosuppression, the systemic inflammatory response, and the
multi-organ dysfunction syndrome. Mortality following thermal injury has decreased in
recent years as a result of the use of new tools and a better understanding of burn
physiopathology. Prompt excision of the burn eschar is reported to prevent mortality after
major thermal injury.
After excision, the surgeon faces a new critical problem - coverage of the burn wound. It
is generally accepted that management of the burn wound involves coverage by means of
autografting. Graft take therefore plays an important role in the survival of burn
patients.
Autografting is the best procedure for the replacement of skin defect due to deep dermal
burn. Currently, textile dressings are frequently preferred for this type of graft.
However, these dressing materials do not fix the graft sufficiently well and may cause
damage to the graft, maceration, and pain in the graft area during dressing changes.
Undoubtedly, graft the take rate is very important for the reduction of mortality and
morbidity in patients with major burn injuries.
In this study, a silicone-coated polyamide dressing material was used as a graft dressing
and its effects on graft take rate were investigated. Silicone-coated polyamide
(Mepitel/SCA Mblnlycke) is an elastic, transparent, non-adherent, porous material. Its
porous structure permits wound exudate to pass directly into absorbent dressings. Mepitel
adheres to dry skin but not to moist wounds.
Materials and methods
Between August 1997 and August 1998,
eighteen patients (mean age, 23 yr; mean burned TBSA 12%) were treated at the G51hane
Military Medical Academy Burn Centre (Turkey). All the patients were treated with a
Mepitel dressing for their graft. Suction compresses were changed on post-operative day 4,
without removal of Mepitel. The compresses were changed until post-operative day 8-12, but
not Mepitel. The graft was easy to observe because of its transparence, and evacuation was
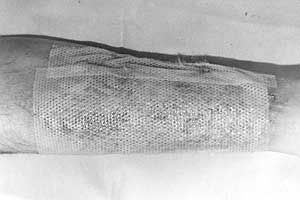
facilitated by its porous structure (Figs 1, 2).
 |
 |
| Fig. la
- Full-thickness burn wound in left lower extremity |
Fig. 1b
- Wound following tangential excision and grafting, with use of Mepitel dressing |
 |
 |
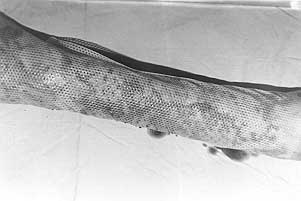
| Fig. lc
- Wound on post-operative day 5. |
Fig. 1d
- Completely healed wound on post-operative day 10. |
 |
 |
| Fig. 2a
- Granulated burn wound on right upper extremity. |
Fig. 2b
- Immediate post-operative appearance of grafted wound with Mepitel dressing. |
 |
Fig. 2c - Wound on post-operative
day 10 |
|
Results
A graft take range of over 90%
was observed in all the grafts, with minimal graft loss in patients receiving a Mepitel
graft dressing. Dressing changes were painless except in four patients when Mepitel did
not adhere sufficiently. Only three patients had a collection of exudate from suppuration,
but the collection was easily evacuated owing to the porous structure, without removal of
Mepitel.
No allergic reaction, maceration, or graft damage was observed.
Discussion
Skin grafting is standard care
in deep dermal burns and also reduces burn-related mortality and morbidity. Graft take is
therefore is very important. In this study, as we have said, we used Mepitel, an elastic,
transparent, porous, non-absorbent material, for graft dressing which improves graft take
rate and reduces pain during dressing changes in children.
An ideal wound dressing should provide a moist, warm, non-toxic, antibacterial, painless,
inexpensive environment for the freshly grafted skin. Most surgeons prefer
petrolatum-impregnated gauze, but this has many disadvantages. A textile dressing may
cause maceration and damage to the graft, as well as pain, especially during the first
dressing changes, and it does not fix the graft adequately. However, Mepitel, which
adheres to dry skin but not to moist graft and wound, was capable of fixing the graft in
flat areas and did not cause maceration or graft damage during compress changes.
Traditionally, all grafts except those in the face are covered with a topical
antimicrobial, using the closed technique. Polysporin/mycostatin ointment is one of the
most common agents. These medications are generally used on a fine mesh gauze. Bulky gauze
dressings and compressive bandages are required for further protection and pressure.
However, some fine-mesh commercial gauzes with various kinds of medication are also
available. Some of these contain Vaseline and antimicrobial agents. Although Mepitel does
not contain any antimicrobial agent, drainage of suppurative material and the application
of antimicrobial agents can be achieved easily, without removal of Mepitel. Chlorhexidine
or petrolatumimpregnated mesh gauzes are other common over-graft dressing materials.
The main goals in the care of patients with partialthickness burns or grafted burn wounds
are the achievement of optimal levels of functionality and cosmesis, with improved wound
healing and pain-free dressing changes Mepitel has been reported to promote wound healing
in patients with partial-thickness burn wounds. We also observed shorter healing periods
for grafted burn wounds in comparison with wounds treated with traditional dressings.
Gotschal et al. reported that Mepitel significantly reduced pain during dressing changes
in burned children. Although Mepitel has not been reported to have any effect on the
bacterial colonization of burn wounds, it was observed that children treated with Mepitel
did not show signs of systemic infection! We observed fewer cases of wound infection in
patients treated with Mepitel.
Although Mepitel has many advantages, it is difficult to apply in concave areas (neck,
axilla) and expensive. It has been reported that Mepitel represents a significant advance
in the treatment of partial-thickness burn wounds. However, although Mepitel may be
considered expensive, it has been reported that overall hospital costs are lower thah
those of traditional dressing materials.
In conclusion, the non-adherent porous dressing Mepitel was found to be highly effective
for graft take and facilitated observation of haernatomas and seromas.
RESUME. L'autogreffe est la meilleure procédure pour fermer les
lésions cutanées causées par les brűlures. Aujourd'hui, en général, on préfčre
l'emploi des pansements textiles. Ces matériaux, toutefois, ne fixent pas trčs bien la
greffe et peuvent causer la macération et une certaine douleur dans la zone de la greffe
pendant les changements du pansement. Dans ce travail, les Auteurs décrivent l'emploi de
pansements polyamides en silicone utilisés pour panser la greffe, et l'effet qu'ils
produisent sur la greffe. Le polyamide revęti de silicone (Mepitel/SCA Môlnlycke) est un
matériau élastique, transparent, poreux et non-adhérent. La structure poreuse de
Mepitel permet ŕ l'exsudat de la lésion de se diffuser directement dans le pansement,
qui adhčre au derme mais non ŕ la lésion humide. Entre mai 1997 et mai 1998, 18
patients soignés au Centre des Brűlés de l'Académie Médicale Militaire Gülhane (âge
moyen, 23 ans; surface corporelle brűlée moyenne, 12%) ont été traités avec l'emploi
de Mepitel comme pansement de la greffe.
Les compresses ŕ succion ont été changées, sans lever le Mepitel, le 4čme jour aprčs
l'opération. Les compresses, mais non le Mepitel, ont été changées jusqu'au 8-12čme
jour post-opératoire. La greffe est facile ŕ observer, ŕ cause de la transparence de
Mepitel, dont la structure poreuse favorise le drainage. Les Auteurs ont observé une
bonne prise de la greffe dans 90% des cas, avec des pertes minimales chez tous les
patients traités avec ce pansement. En conclusion, selon les Auteurs, le pansement
Mepitel, non-adhérent et poreux, se montre efficace pour la prise de la greffe et
favorise l'observation des hématomes et des séromes.
BIBLIOGRAPHY
- Selmanpakoglu N., Oztan 0., Deveci M.,
Sengezer M.: Clinical application of skin homograft for extensive burns. Turk. J. Plast.
Surg., 1: 98-102, 1993.
- Chih-chun Y., Tsi-siang S., We-shia
X.: A Chinese concept of treatment of extensive third-degree burns. Plast. Reconstr.
Surg., 70: 238, 1982.
- Munster A.M.: The immunological
response and strategies for intervention. In: Herndon D. (ed.): "Total Burn
Care" (2nd edition), W.B. Saunders Co., Philadelphia, 279-92, 1996.
- Muller J.M., Nicolai M., Wiggins R.,
Macgill K., Hemdon D.: Modem treatment of a burn wound. In: Hemdon D. (ed.): "Total
Burn Care" (2nd edition), W.B. Saunders Co., Philadelphia, 136-47, 1996.
- Burke J.F., Quinby W.C., Bondoc C.C.,
Cosimi A.B., Russell P.C.: Immunosuppression and temporary skin transplantation in the
treatment of massive third-degree burns. Ann. Plast. Surg., 182: 183, 1975.
- Heimbach D.M.: Early excision and
grafting. Surg. Clin. North Am., 67: 93-107, 1987.
- Gotschall C.S., Morrison M.I.,
Eichelberger M.R.: Prospective randomized study of efficacy of Mepitel on children with
partialthickness scalds. J. Burn Care Rehabil., 19: 279-83, 1998.
This paper was
received on 1 November 1998.
Address correspondence to:
Dr M. Deveci
Department of Plastic and Reconstructive Surgery and Burn Centre
Gillhane Military Medical Academy, Turkey. |
G. WHITAKER
INTERNATIONAL BURNS PRIZE
PALERMO, ITALY
Under the patronage of the
Authorities of the Sicilian Region for 2000
By law n. 57 of June 14th 1983
the Sicilian Regional Assembly authorized the President of the Region to grant the
Giuseppe Whitaker Foundation, a non-profit-making organization under the patronage of the
Accademia dei Lincei with seat in Palermo, an annual contribution for the establishment of
the G. Whitaker International Burns Prize aimed at recognizing the activity of the most
qualified experts from all countries in the field of burns pathology and treatment.
The amount of the prize is fixed at twenty million Italian lire. The prize will be awarded
every year by the month of June in Palermo at the seat of the G. Whitaker Foundation.
The Adjudicating Committee is composed of the President of the Foundation, the President
of the Sicilian Region, the Representative of the Accademia dei Lincei within the G.
Whitaker Foundation, the Dean of the Faculty of Medicine and Surgery of Palermo
University, the President of the Italian Society of Plastic Surgery, three experts in the
field of prevention, pathology, therapy and functional recovery of burns, the winner of
the prize awarded in the previous year, and a legal expert nominated in agreement with the
President of the Region as a guarantee of the respect for the scientific purpose which the
legislators intended to achieve when establishing the prize.
Anyone who considers himself/herself to be qualified to compete for the award may send by
January 3 1 st 2000 a detailed curriculum vitae to: Michele Masellis M.D.,
Secretary-Member of the Scientific Committee G. Whitaker Foundation, Via Dante 167, 90141
Palermo, Italy. |
|