Annals of Burns and Fire Disasters - vol. XII - n° 2 - June 1999 EXPANDED SUPRACLAVICULAR ARTERY ISLAND FLAP FOR POST-BURN NECK RECONSTRUCTION Abdel-RazekPlastic, Reconstructive and Burns Unit, Tanta Faculty of Medicine, Tanta, Egypt SUMMARY. Burn scar contractures involving the anterior neck represent a surgical problem for the plastic and reconstructive surgeon. To improve functional and cosmetic results we used a new technique by means of which we obtained a large amount of skin with the same functional and cosmetic properties as neck skin. This new idea consists of expansion of the supraclavicular area supplied by the supraclavicular artery, followed by transmission of the expanded fasciocutancous flap based on the same artery as an island flap to cover the anterior neck after release and excision of post-burn scars. This technique was used in eleven patients suffering from postburn mentosternal contracture. All the flaps healed primarily with good functional and cosmetic results, and the donor sites closed primarily without any tension. Introduction Mentosternal contractures represent a surgical challenge to the plastic and reconstructive surgeon. The challenge lies in the restoration of the form and function of this region. The traction forces caused by burn scar contracture may pull the chin, cheeks, and lower lip caudally, resulting in incomplete oral occlusion and cicatricial ectropion, in addition to possible tracheal alterations affecting respiration and to distortions of the cervical spine.In the growing child, scar contractures in the cervical region impair mandibular growth, and early operative correction is generally recommended. Acute deep burns in the neck are best managed with split-thickness skin graft and extension splinting for a period of six months. Many surgical procedures havIe been used to correct these contractures, including free skin grafts, local flaps with or without tissue expansion, and free flaps. To achieve good functional and cosmetic results the operative procedure should fulfil the cosmetic and functional criteria of the neck. This paper describes the addition of an expansion to the supraclavicular island flap described by Pallua et al., in which we placed a tissue expander under the flap in order to give greater width and length to the flap and to facilitate easy closure of the donor site. Surgical anatomy Fresh cadaver dissection performed by Lamberty on the supraclavicular flap found that the arterial supply of the flap is the superficial branch of the superficial transverse cervical artery - subsequently named the supraclavicular artery. The arterial vessels range from 1.0 to 1.5 min in diameter and are constantly joined by one or two major concomitant veins. These vessels emerge beneath or lateral to the posterior belly of the omohyoid muscle (Fig. 1).
It has to be taken into account that the distal portion of the flap may be perfused in retrograde fashion by branches of the posterior circumflex humoral artery through ariastomoses over the point of the shoulder. Injection studies showed that the flap can be raised with dimensions of up to 30 cm in length and 12 cm in width. Patients and methods Between July 1997 and October 1998 eleven patients with post-burn neck contracture were operated upon using an expanded supraclavicular artery island flap for resurfacing the neck after release and excision of post-burn neck contractures. Flap design and expander application
Under general anaesthesia an incision was made in the infraclavicular area, 4 cm in length and 2 cm below the proposed anterior border of the flap. Dissection was performed underneath the flap, below the deep fascia, in order to create a pocket for insertion of the expander. A 300 cc rectangular tissue expander was inserted into the pocket. The inflating tube exited through a separate stab at the distal border of the proposed flap, which at the same time effected tube drainage. Inflation of the expander was performed immediately intra-operatively to a degree that closed the dead space (Fig. 3).
After two weeks we started expansion three times weekly until we reached the desired expansion (Fig. 4). The patient was then re-operated upon, and the contracted bands and disfiguring scars were removed, up to the borders of the aesthetic unit, until the neck was fully raised on its vascular pedicle, permitting a 180° angle of rotation (Figs. 5a,b). Haemostasis was performed, the expander was removed, and the flap was raised with the capsule intact in order to protect the axially running supraclavicular vessels reaching the medial part of the flap. Care was be taken to avoid injury to the accessory nerve and the pedicle, which mostly arise from the superficial transverse cervical artery.
Positioning
of the flap (Fig. 6)
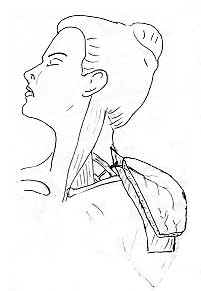
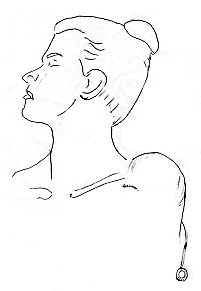
Donor site closure Results Between July 1997 and October 1998 eleven patients with post-burn neck contracture were operated upon in the Tanta University Plastic and Reconstructive Surgery Unit in Egypt. Nine of the patients were female and two male. The age range was from 16 to 36 yr. The degree of contracture was severe in nine patients, while two presented neck scarring and hypopigmentation with a mild degree of neck contracture (Figs. 7, 8a,b).
All the
donor sites healed by primary intention, and all the flaps survived completely, with just
one presenting distal congestion at the end of the operation, when superficial sloughing
of the part occurred with some effect on the cosmetic outcome. One patient complained of
minor scar contracture at the proximal end of the flap, and this was corrected by Z-plasty
under local anaesthesia. Another minor complication was haematoma under the flap in a
patient in whom the drainage system was obstructed by blood; in this case evacuation of
the haematoma was performed under general anaesthesia and a widepore drainage system was
used, after which the flap survived without further problems. Dehiscence of the suture
line during inflation of the expander occurred in one patient, and in this case we
inflated the expander for one week and then performed the second stage. Discussion Burn scar contracture
involving the anterior cervical neck presents a unique set of problems compared with the
rest of the body. The challenge lies in the restoration of the form and function of this
body region. The skin of the neck is thin and pliable and because of the neck's
flexibility it is prone to the formation of contractures, which not only affect the
movement of the neck but can also affect the function of the lower face. The application
of tissue expansion to a flap is a further refinement of two well-known flaps, a method
stumbled upon by TansinP late last century and rediscovered by Olivari.
Pallua et al. avoided
these disadvantages by raising the flap as an island flap rotated up to 180° in order to
cover the defect, and the donor site was closed primarily after extensive dissection. Zaki
presented his experience in the management of post-burn neck contracture using the
supraclavicular island flap. He used the bilateral flap in patients with extensive neck
scarring and gave the flap a new name (Epaulet flap). Conclusion The supraclavicular island flap is a very useful flap for neck reconstruction as it is safe and easy to elevate and offers greater mobility and rotation owing to the isolation of the vascular pedicle. It also provides a good colour match. The modification that we added to the application of the tissue expander appears to be useful as it produces a large thin flap that can be used to fill considerable defects, yet still allowing the donor site to be closed directly.
RESUME. Les contractures dues aux cicatrices des brűlures qui intéressent la zone du cou antérieur constituent un problčme pour la chirurgie plastique et reconstructive. Pour améliorer les résultats fonctionnels et cosmétiques les Auteurs ont employé une nouvelle technique qui a permis d'obtenir une grande quantité de derme ayant les męmes proprietés fonctionnelles et cosmétiques de la peau du cou. Cette nouvelle idée consiste dans l'expansion de la zone supraclaviculaire alimentée par l'artčre supraclaviculaire, suivie par la transmission du lambeau fasciocutané soumis ŕ l'expansion basé sur la męme artčre que le lambeau en îlot pour couvrir le cou antérieur aprčs la libération et l'excision des cicatrices dues aux brűlures. Les Auteurs ont employé cette technique dans 11 patients atteints de contractures mentostemales causées par les brűlures. Ils ont obtenu la cicatrisation primaire de tous les lambeaux avec de bons résultats fonctionnels et cosmétiques et avec la fermeture primaire des sites donneurs sans aucune tension. BIBLIOGRAPHY
|
|||||||||||||||||||||||||||