Annals of
Burns and Fire Disasters - vol. XII - n° 2 - June 1999
AETIOLOGIES AND OUTCOMES OF BURNS IN INFANTS
UNDER ONE YEAR OLD
Arsian E., Dalay C., Qinaroolu E., Aksoy M.K, Acartúrk S.
Department of Plastic and Reconstructive Surgery and Burn Unit, Qukurova
University Medical School, Adana, Turkey
SUMMARY. Between January 1993 and December 1997,
711 burn victims were hospitalized in the Burns Care Unit of Balcali Hospital in Adana,
Turkey, of whom 39 (5.48%) were under 12 months old. Of these 39 infants (mean aged 9 ±
0.5 months ± S EM), 26 were male and 13 female. Burn extent ranged between 5 and 9 1 % T
BSA. The main aetiological factors were hot water and mi lk scalds, fl ame, and
electricity. There were 11 deaths overall (28.20%). The mortality rate was 37.5% among
infants aged 0-6 months and 25.801 among infants aged 7-12 months. The mean burn extents,
in these two age groups, were respectively 22.87% and 20.25%. The mortality rate was
58.33% in burns > 25 % and 85.71% in burns > 30 %. The results indicate that burns
in infants are serious traumas and have higher mortality rates than in other age groups.
As infant burns are preventable, education of the parents is a basic requirement.
Introduction
Burn
injury is a trauma common to all age groups, but paediatric patients constitute a large
part of them. A review of the literature revealed many reports on burned children. There
are papers on aetiology, outcome, epiderniology, risk factors, burn repeated burns, and
prognostic scores of burns in paediatric age groups. The term "paediatric age
group" is variously defined as that under 16 years and under 19 years, but in this
paper we will seek to evaluate paediatric burn patients up to the age of one year, i.e.,
children who are non-walkers. Burn traumas in this age group are not so rare as might be
expected, and the outcome is often poor. Parental negligence is the main cause of
paediatric burn trauma and this type of burn is therefore easily preventable.
Patients and methods
Between
January 1993 and December 1997, 711 burn victims were hospitalized in the Burns Care Unit
at Balcali Hospital in Adana, Turkey. Of the 711 patients, 39 were under 12 months old.
The age, sex, cause of burn, cause of death, and mortality rate were tabulated and
analysed. The percentage of total body surface area (TBSA) burn involvement was estimated
by the burn team doctor according to the Lund and Browder chart.
All patients received standardized care. Fluid resuscitation was carried out according to
the Parkland formula. Escharotomy was performed under general anaesthesia when indicated.
For daily burn wound dressings, silver sulphadiazine was used. After fluid resuscitation
and stabilization of the patient, early excision of deep burn areas was performed on day 3
or 4 postburn. No prophylactic antibiotics were normally given (antibiotics were only
given according to sensitivity profiles in the presence of positive wound and/or blood
cultures).
Results
Of the
39 infants (mean age: 9 ± 0 .5 months), 26 were male and 13 were female, (maleffetriale
ratio, 2 to 1). The males were slightly younger (inewa age, 9 ± 0.7 months; range, 1-12
months) than the females (mean age, 10 ± 0.6 months; range 6-12 months). Burn extent
ranged between 5 and 91% T13SA, (21 ± 3%). Burn extent in males (mean, 18 ± 2%; range,
5-44%) was slightly less than in females (mean, 26 ± 6%; range, 6-91%).
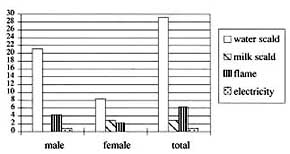
The aetiological factors were hot water scalds (29/39 = 74%), hot milk scalds (3/39 = 8%),
flame (6/39 = 1 5%), and electricity (l/39 = 3%). In males, the aetiological factors were
hot water scalds (21/26 80.26%), flame (4/26 = 15.38%), and electricity (l/26 3.84%) and,
in females, hot water scalds (8/13 = 61.53%), hot milk scalds (3/13 = 23.07%), and flame
(2/13 = 15.38%) (table I). Burn extent according to aetiology is shown in TableII.
|
|
Table I - Aetiological
factor |
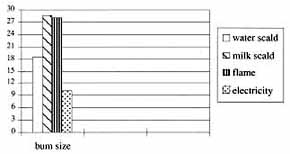
Table II - Burn size (% TBSA)
according to aetiological factors |
|
Burn
size was greater in scalds with hot milk and flame (respectively, 28.33 ± 10.84% and
28.17 ± 13.86%) than in scalds with hot water and electricity (respectively, 18.86
±1.69% and 10%). There were 11 deaths overall (11/39 = 28.20%), six in boys. The causes
of death were hot water scalds (7/11 = 63.63%), flame (2/11 = 18.18%), and hot milk scalds
(2/11 = 18.18%) (Table III).
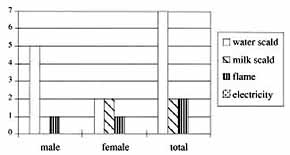 |
Table III - Deaths according to aetiological factors |
|
The
deceased infants were aged between 3 and 12 months (mean age, 9.36 ± 0.96 months). The
mortality rate among infants aged 0-6 months was 3/8 (37.5%) and among infants aged 712
months 8/31 (25.8%). The mean burn extents in the same age groups were respectively 22.87%
and 20.25%. The mortality rate was 58.33% in burns > 25% and 85.71% in burns > 30%.
Discussion
All these infants were non-walkers. The main cause of the burn
trauma was the parents negligence, particularly that of the mothers, who spend more time
with children than fathers. In our study, all the mothers were housewives spending most of
their time at home. As these infants were unable to walk, it cannot be accepted that they
caused the burn trauma themselves, even accidentally. In parents' education programmes the
importance of proper care must be strongly emphasized.
Of the infants, four were aged bet~,veen 10-12 months and were in their baby-walkers when
the accident occurred. The aetiology in these children was scalding with hot water
prepared for five o'clock afternoon tea. The risks presented by baby-walkers was recently
described by Cassell et al., 2 who recommend a ban on this potentially dangerous device.
We are not sure that any kind of ban could prevent such accidents but we believe that
parents, and in particular mothers, should be made aware of the sort of trauma that
infants have to face when they are iri walkers. Children should be kept in bed or in their
own room at home. Sleeping children are out of danger if they are not in the kitchen.
Children must be put in the.ir bedrooms when asleep and in a safe place, excluding the
kitchen, while the mother is cooking or performing routine housework chores.
In families of lower social an6 economic status, especially in villages in Turkey, it is a
customary action to heat milk in large boilers in the garden of the house. This is another
potential source of dangerous burn trauma. It may be difficult to give up this
long-standing practice, but people must learn to keep children out of the garden while
milk is boiling. As an aetiological factor scalding with boiling milk is generally rare,
an6 a study performed by Bang and Ghoneim" reported only one case due to this cause.
In our study, this cause was ri.-sponsible in three cases (7.69%), with a mortality rate
cf 66.7%. The high mortality is particularly noticeable. PaTents must therefore do their
utmost to prevent these accidents from happening, just as physicians must manage their
treatment with all possible care.
A crawling child must be kept under control and not be permitted to leave its room or
wander around the house where there is no danger of burn trauma. If the child is left
unattended, it may move towards a potential cause of burn trauma. In all cases, parental
negligence is central to burn accidents in non-walking infants.
Our patients present a high mortality rate. We are unable to compare our results with
thDse of other series as there is no similar study dealing with non-walkers. When the mean
extent of 20.79 ± 2.53% TBSA and the mortality rate of 28.20% in the infant age group are
considered together, it seems that the mortality rate among infants is higher than in any
other age group. Our mortality rate of 28.20% was similar to that reported by Bang and
Ghoneim 14 (28.40%)
and lower than that reported by Hamit (40.9%), Yoshioko(42.2%), Haberal (35.7%) and
Reig (30.7%). The main difference between the studics concerns the age groups and the mean
percentage of TBSA burned. Our mortality rate for burns was 58.33% in burns > 25% TBSA
and 85.71% for burns > 30% TBSA. These figures are higher than that of 48.2%, even for burns > 40% TBSA reported by Bang and
Ghoneim and that of
35.7% reported by Benmeier. With regard to mortality rates versus
affected TBSA, our results are somewhat poor. We can defend ourselves us by pointing out the nature of our different and handicapped age
group.
Like burns of all aetiologies and in all age groups,
burns in non-walkers are certainly preventable traumas. When a burn trauma occurs in a
non-walker, it not only the child that is hurt but also society, owing to the increased
need of resources to pay for protracted hospital admission and to the high mortality rate.
RESUME.
Entre janvier 1993 et décembre 1997, les Auteurs ont traité 711 patients
brűlés dans l'Unité des Brűlures ŕ Adana, Turquie. De ces patients 39 (5,48%) étaient
âgés moins de 12 mois (âge moyen, 9 ± 0,5 moins) (± ESM), dont 26 mâles
et 13 femelles. L'extension moyenne de la brűlure variait entre 9 et 91%
de la surface corporelle totale. Les facteurs étiologiques principaux étaient les
ébouillantements par l'eau et le lait chaud, les flammes et l'électricité. Le numero
total des décčs était Il (28,20%). Le taux de mortalité était 37,5% entre
les enfants âgés de 7 ŕ 12 mois. L'extension moyenne des brűlures, dans
les deux groupes, était respectivement 22,78% et 20,25%. Le taux de
mortalité était 58,33% pour les brűlures > 2 5l'/c et 85,71% pour
les brűlures > 30 %. Les résultats indiquent que les brűlures dans les
enfants constituent des traumatismes graves et portent ŕ des taux (le mortalité plus
élevés des brűlures dans les autres groupes d'âge. Puisque les brűlures en âge
pédiatrique sont évitables, l'éducation des parents est une nécessité absolue.
BIBLIOGRAPHY
- Morrow S.E., Smith D.L., Cairns B.A.,
Howell P.D., Nakayama D.K., Peterson H.D.: Etiology and outcome of pediatric burns. J.
Pediatr. Surg., 31: 329-33, 1996.
- Cassell O.C., Hubble M., Milling M.A.,
Dickson W.A.: Baby walkers - still a major cause of infant burns. Burns, 23: 451-3, 1997.
- Sarma B.P., Sanna N.: Epidemiology,
mortality and treatment of burn injuries - a study in a peripheral industrial hospital.
Burns, 20: 253-5, 1994.
- Mercier C., Blond M.H.:
Epidemiological survey of childhood burn injuries in France. Burns, 22: 29-34, 1996.
- Hummel R.P., Greenhalgh D.G., Barthel
P.P., De Sema CM, Gottschlich M.M., James L.E., Warden G.D.: Outcome and socioeconomic
aspects of suspected child abuse scald burns. J. Burn Care Rehabil., 14: 121-26, 1993.
- Saffle J.R., Davis B., Williams P.:
Recent outcomes in the treatment of burn injury in the United States: a report from the
American Burn Association Patient Registry. J. Burn Care Rehabil., 16: 219-32, 1995.
- Herruzo Cabrera R., Fernandez Arjona
M., Garcia Torres V., Martinez Ratero S., Lenguas Portero F., Rey Calero J.: Mortality
evolution study of burn patients in a critical care burn unit between 1971 and 1991.
Burns, 21: 106-9,1995.
- Kumar P., Sharma M., Chadha A.:
Epidemiological determinants of burns in paediatric and adolescent patients from a centre
in western India. Burns, 20: 236-40, 1994.
- Dedovic Z., Brychta P., Koupilova I.,
Suchanek I.: Epidemiology of childhood burns at the Burn Centre in Bmo, Czech Republic.
Burns, 22: 125-9, 1996.
- Forjuoh S.N., Guyer B., Strobino D.M.,
Keyl P.M., Diener West M., Smith G.S.: Risk factors for childhood burns: a case control
study of Ghanaian children. J. Epidemiol. Community Health, 49: 189-93, 1995.
- Forjuoh S.N.: Burn repetitions in
Ghanaian children: prevalence, epidemiological characteristics and socioenviionmental
factors. Burns, 22: 539-42, 1996.
- Demirdjian G.: Adjusting a prognostic
score for burned children with logistic regression. J. Burn Care Rehabil., i 8: 313-6,
1997.
- Greenhalgh D.G., Housinger T.A., Kagan
R.J., 1:16cman M., James L., Novak S., Farmer L., Warden G.D.: Maintenance of serum
alburnin levels in pediatric burn patients: a prosp(~ctive, randomized trial. J. Trauma,
39: 67-73, 1995.
- Bang R.L., Ghoneim I.E.: Epidemiology
and moitality of 162 major burns in Kuwait. Burns, 22: 433-8, 1996.
- Hamit H.F.: Factors associated with
deaths of burn patients in a community hospital. J. Trauma, 18: 405, 1978.
- Yoshioko T., Ohashi Y., Sugimoto H.,
Sawada Y., Kobayashi H., Sugimoto T.: Epidemiological analysis of deaths caused by burns
in Osaka, Japan. Burns, 8: 414-23, 1982.
- Haberal M., Oner Z., Bayraktar U.:
Epidemiology of adults and children burns in a Turkish burn center. Burns, .3: 136-40,
1987.
- Reig A., Tejerina C., Baena P.,
Mirabet V.: MasAve burns: a study of epidemiology and mortality. Burns, 20: 51-54, 1994.
- Benmeier P., Sagi A., Greber B. et
al.: An anal) sis of mortality in patients with burns covering 40 per cent 13SA or more: a
retrospective review covering 24 years (1964-88). Burns, 17: 4025, 1991.
This paper was received on 4 November
1998.
Address correspondence to: Dr Emrah Arslar
Cukurova Universitesi Tip Fakultesi, Plastik Ve Rekonstruktif Cerrahi A.D.
01130, Adana, Turkey
(fax: 90 322 338 6427). |
|