Annals
of Burns and Fire Disasters - vol. XII - n° 2 - June 1999
ACUTE COLONIC
PSEUDO.OBSTRUCTION (OGILVIE'S SYNDROME) - A RARE COMPLICATION OF SEVERE THERMAL INJURY.
REPORT ON TWO CASES
Tsoutsos D, Tsakou EG, Lykoudis E,
Stamatopoulos C, Tatoulis R, loannovich J.
Department of Plastic Reconstructive Surgery and Burns Centre, G. Germhmataz
General State Hospital of Athens, Greece
SUMMARY. Two cases of acute colonic
pseudo-obstruction (Ogilvie's syndrome) in patients with extensive burns arc presented.
Tile clinical symptoms, diagnostic approach, and therapeutic measures are analysed and
discussed in relation to their impact on burn patient survival and outcome.
Introduction
Acute pseudo-obstruction of the colon
(Ogilvie's syndrome) is characterized by a dramatic dilatation of the colon in the absence
of any mechanical obstruction. The condition mainly affects the caecum and right colon,
and can lead to life-threatening perforation.
Ogilvie's syndrome is attributed to autonomous nervous system imbalance, but the
pathogenic mechanism remains unknown. It can complicate thermal injuries and several other
intra- and extra-abdominal disorders (Table 1).
| Systemic |
|
Cardiovascular |
|
| |
Metabolic |
|
Heart failure |
| |
Electrolyte imbalances |
|
Myocardial infarction |
| |
Alcoholism,drugs |
|
Pulmonary embolism |
| |
Infection,sepsis |
Retroperitoneal |
|
| |
Pregnancy and delivery |
|
Haemorrhage |
| |
Old age |
|
Pyelonephritis |
| |
Cancer |
Post-operative |
|
| |
Uraemia |
|
Caesarean section |
| |
Hypothyroidism |
|
Spinal cord operation |
| Neurological |
|
|
Orthopaedic operation |
| |
Parkinsonism, dementia |
|
Intra-abdominal operation |
| |
Spinal cord diseases |
Abdominal infection |
|
| |
Brain tumours |
|
Pancreatitis |
| Traumatic |
|
|
Cholecystitis |
| |
Intra- or extra-abdominal |
Burns |
|
|
| Table I - Conditions associated with Ogilvie's
syndrome |
Although the
syndrome occurs only rarely, it greatly increases burn patient mortality, and in the
presence of the relative symptoms a high level of suspicion is recommended.
The incidence of the syndrome in burn patients is estimated to be I %.'In the last five
years, of the 422 patients with over 15% burns treated in our burn unit, two patients
developed the syndrome, with an incidence of 0.47%.
Case reports
Case 1
A 62-year-old male presented with 55% T13SA partial- and full-thickness burns with
associated inhalation injury. There was no past medical history of note, apart front gross
obesity.
On the third day post-burn the patient developed pneumonia, associated with severe hypoxia
and respiratory alkalosis, which required endotracheal intubation and supported
ventilation. Additionally, he developed severe thromboeytopenia (plt = 3,000/ml).
On the same day he also developed rapidly increasing abdominal distension, pyrexia (38
'C), increased respiratory distress, and obstipation Bowel sounds were absent. Abdominal
x-ray in the lateral decubitus position revealed marked distension of the entire colon
(Fig. 1).
 |
Fig. 1 - Abdominal x-ray in
lateral decubitus position. Marked distension of entire colon. |
|
Owing to the patient's poor
condition a conservative approach was elected, consisting of: a. insertion of a largebore
nasogastric tube, which produced a copious amount of gastric fluid; b. diagnostic and
therapeutic colonoscopy, which showed no evidence of mechanical obstruction and
temporarily decompressed the colon; and c. insertion of a colonic decompression tube,
which was left in place in order to provide continuous mechanical relief.
On the fifth day post-burns the patient deteriorated rapidly, showing evidence of
respiratory failure, generalized peritonitis, and sepsis. He died the following day.
Autopsy revealed generalized peritonitis due to perforation of the markedly dilated and
necrosed colon.
Case 2
A 53-year-old male presented with a 37% T13SA fullthickness burns and associated
inhalation injury. He was a heavy smoker and had a history of advanced chronic obstructive
pulmonary disease and hypertension.
During his hospitalization he developed hypoxia and severe hyperglycaemia. On the 16th
post-burns day he presented abdominal distension, vomiting, pyrexia (38.3 °C), mild
abdominal pain, and diarrhoea. Erect abdominal x-ray revealed excessive dilatation of the
colon with concomitant air fluid levels (Fig. 2). Immediate treatment included: a.
insertion of a nasogastric aspiration tube; b. colonoscopy, which failed to reveal
mechanical obstruction and to decompress the bowel; and c. insertion of a colonic
decompression tube.
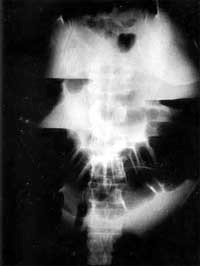 |
Fig. 2 - Abdominal x-ray in erect
position. Excessive dilatation of colon with concomitant air fluid levels. |
|
The patient was checked
with frequent abdominal xrays, which showed increasing colonic distension. When the caecal
diameter exceeded 12 cm, an immediate laparotomy was performed.
The operative findings included an enormously dilated colon with a small area of focal
necrosis in the caecum, but no perforation (Fig. 3). Consequently, a subtotal
colectomy with temporary ileostomy was performed. Apart from three surgical operations for
resurfacing the burn area with partial -thickness skin grafts the patient's further
hospitalization was uneventful. He was discharged on the 53rd post-burn day. The ileostomy
was reversed two months later, since when he has been fit and well.
 |
Fig. 3 - Operative findings.
Enormously dilated colon with small area of focal necrosis in caecum, but no perforation. |
|
Discussion
Acute colonic pseudo-obstruction as a
syndrome was first described by Ogilvie in 1948.'It is characterized by colonic dilatation
in the absence of mechanical obstruction or any obvious causes of paralytic ileus. The
syndrome's pathogenic mechanism remains unknown.
Until 1986 only 400 cases had been reported. The condition can occur in patients with
various metabolic, surgical, and medical problems. It can also be idiopathic in a small
percentage of patients.
With regard to the syndrome's common presenting symptoms (Table II), both our
patients had sudden and rapidly increasing abdominal distension, respiratory distress, and
moderate fever. The first patient had obstipation and reduction of bowel sounds, while the
second had diarrhoea, mild abdominal discomfort, and increased bowel sounds. Both patients
received total enteral nutrition, prior to the development of the syndrome, via a
nasoduodenal tube and a controlled administration pump. Enteral nutrition is not
considered to contribute to the manifestation of the syndrome, as proved by its uneventful
administration to burns patients in our clinic with TBSA exceeding 15%. Both had
inhalation injury, infection, and severe hypoxia, which may have triggered the development
of the syndrome.
| Abdominal distension |
100% |
| Abdominal pain |
83% |
| Nausea |
63% |
| Vomiting |
57% |
| Constipation |
51% |
| Diarrhoea |
41% |
| Pyrexia |
37% |
|
| Table II - Common presenting symptoms of Ogilvie's syndrome
on the basis of the analysis of 400 cases (Vane K.V., Al-Salti M.) |
The common symptoms and signs of the syndrome (e.g.,
tympany, increased or decreased bowel sounds, tachycardia, pyrexia, increased number of
leucocytes in peripheral blood, and severe abdominal pain) may be difficult or impossible
to evaluate in severely burned patients.
The appearance of sudden and rapidly increasing abdominal distension therefore
necessitates subsequent frequent evaluation with a series of abdominal x-rays, preferably
in the erect position, if the condition of the patient permits. The presence of diffuse
colonic dilatation, with or without air fluid levels or free air, in the event of
perforation, can be detected. Treatment consists of conservative measures, colonoscopy,
and surgery.
Conservative treatment should include insertion of a nasogastric aspiration tube,
cessation of food ingestion, insertion of a colonic decompression tube, discontinuation of
narcotic analgesics, early correction of fluid and electrolyte imbalance, and control of
systemic disturbances.
Colonoscopy at the earliest possible time can be of both diagnostic and therapeutic value
as it provides: a. exclusion of obstruction and establishment of the diagnosis among other
possible causes of colonic dilatation (Table III) and b. successful decompression
of the colon in up to 81% of the patients.
| * Colonic volvulus |
| * Bowel obstruction |
| * Paralytic ileus |
| * Acute gastric distension |
| * Acute abdomen |
| * Ischaemic bowel |
|
| Table III
- Differential diagnosis of Ogilvie's syndrome |
The recurrence rate of
dilatation is high, as happened in our first case. In an enormously dilated colon,
colonoscopy can be hazardous and should therefore be avoided.
There is no consensus regarding the value of gastrointestinal motility drugs such as
neostigmine, metinclopramide, urecholine, and cicapride.
Indications for immediate operative intervention are: a. signs of bowel wall necrosis or
peritonitis; b. caecal diameter greater than 12 cm in erect x-rays; failure of
conservative management; d. severe respiratory embarrassment; and e. impossibility of
excluding mechanical obstruction of the colon.
In cases with no rupture or in the absence of massive colonic dilatation with ischaernia,
surgical decompression of the colon can be accomplished via caecostomy or Colostomy. In
cases with perforation or ischaernia, which can lead to perforation of the colonic wall,
partial or subtotal colectomy is indicated with immediate or delayed restoration of
intestinal continuity, depending on the patient's condition.
In conclusion, Ogilvie's syndrome is a rare but serious complication in burns patients.
The outcome depends mainly on early detection and prompt treatment of the syndrome.
RÉSUME. Les Auteurs
présentent deux cas de pseudo-obstruction aiguë du côlon (syndrôme d'Ogilvie) dans des
patients atteints de brűlures étendues. Aprčs avoir analysé les symptômes cliniques,
l'approche thérapeutique et les résultats obtenus, ils discutent leur effet sur la
possibilité de survie des patients et les résultats finals.
BIBLIOGRAPHY
- Nanni G. et al.: Ogilvie's syndrome (acute colonic pseudo
obstruction). Dis. Colon and Rectum, 25: 157-66, 1982.
- MacColl C., MacCannell K. et a].: Treatment of acute
colonic pseudo-obstruction with cicapride. Gastrenterology, 98: 773-6, 1990.
- Vane K.V., Al-Salti M.: Acute colonic pseudo-obstruction
(Ogilvie's syndrome). Dis. Colon and Rectum, 29: 203-10, 1986.
- Lescher T. et a].: Acute colonic pseudo-obstruction in
thermally injured patients. Dis. Colon and Rectum, 21: 618-22, 1978.
- Geelhoed G.: Colonic pseudo-obstruction in surgical
patients. Am. J. Surg., 149: 258-65, 1985.
- Arranz C., Garcia de Tena et al.: Prolonged colonic
pseudoobstruction (Ogilvie's syndrome) in an older woman resolved with conservative
treatment. J. Am. Geriatr. Soc., 44: 1016-7, 1996.
- Martin F.M., Robinson A.M. et aL: Therapeutic colonoscopy
in the treatment of acute colonic pseudo-obstruction. Am. Surg., 54: 51922, 1988.
- Clarke H.D., Berry D.J. et al.: Acute pseudo-obstruction of
the colon as a post-operative complication of hip arthroplasty. J. Bone Joint Surg. Am.,
79: 1642-7, 1997.
- Ogilvie H.: Large-intestine colic due to sympathetic
deprivation: a new clinical syndrome. Br. Med. J., 2: 671-3, 1948.
- Gasala V. et al.: Acute colonic pseudo-obstruction in a
burns patient. Burnss, 19: 538-40, 1993.
- Bachulis B., Smith P.: Pseudo-obstruction of the colon. Am.
J. Surg., 136: 66-72, 1978.
- Melzig E.P., Terz J.: Pseudo-obstruction of the colon.
Arch. Surg., 113: 1186, 1978.
- Attiyeh F., Knapper W.: Pseudo-obstruction of the colon
(Ogilvie's syndrome). Dis. Colon and Rectum, 23: 106-8, 1980.
- Bode W., Beart R. et al.: Colonoscopic decompression for
acute pseudo-obstruction of the colon (Ogilvie's syndrome). Am. J. Surg., 147: 243-5,
1984.
- Kukova J.S., Dent T.L.: Colonoscopic decompression of
massive non-obstructive cecal dilatation. Arch. Surg., 112: 512-7, 1977.
- Nivatrongs S., Vermelen F.D., Fang D.T.: Colonoscopic
decompression for acute pseudo-obstruction of the colon. Am. Surg., 196: 598, 1982.
- Sariego J. et al.: Colonoscopically guided tube
decompression in Ogilvie's syndrome. Dis. Colon and Rectum, 34: 720, 1991.
- Norton L., Young D., Scribner R.: Management of pseudo
obstruction of the colon. Surg. Gynecol. Obstet., 138: 595, 1974.
- Nakhgerany K.B.: Colonoscopic decompression of the colon in
patients with Ogilvie's syndrome. Am. J., Surg., 148: 317, 1984.
- Strobel W.E. et a].: Therapeutic and diagnostic colonoscopy
in non obstructive cooling dilatation. Ann. Surg., 197: 416-21, 1983.
- Milo R.: Non-cholinergic non-antidopaminergic treatment of
chronic digestive symptoms suggestive of a motility disorder. Curt. Ther. Res., 36:
1053-62, 1984.
- Schurkes S., Van Nueten J. et al.: Motor stimulating
properties of cicapride on isolated gastrointestinal preparations of the guinea pig. J.
Phann. Exp. Ther., 234: 775-83, 1985.
- Anuras S., Shirari S.: Colonic pseudo-obstruction. Am. J.
Gastroenterology, 79: 525, 1984.
- Adams J.T.: Adynamic ileus of the colon: An indication for
cecostomy. Arch. Surg., 109: 503, 1974.
- Lowman R.M., Davis L.: An evaluation of cecal size in
impeding perforation of the cecum. Surg. Gynecol. Obstet., 103: 711, 1956.
- Spira I.A., Wolff W.I.: Pseudo-obstruction of the colon.
Am. J. Gastroenterology, 65: 397-408, 1976.
Baker D.A., Morin M.E. et al.: Colonic
ileus: indication for prompt decompression. JAMA, 241: 2633-4, 1979.
This paper was received
on 18 January 1999.
Address correspondence to:
Dr D. Tsoutsos
Department of Plastic Reconstructive Surgery and Burns Centre
G. Gennhmataz General State Hospital of Athens, Greece. |
|