Annals of
Burns and Fire Disasters - vol. XII - n° 3 - September 1999
BURNS: THE
IMPORTANCE OF THE DOMESTIC ENVIRONMENT
Santos Heredero F.X.,ą Jiménez Garcia R.,˛
Sŕnchez-Gabriel Lopez J.,ą Martinez Hernŕndez D.,˛ Arroyo Romo C.,ą
Hamann C.ą
Hospital Universitario del Aire, Madrid, Spain
ą Plastic Surgery Department
˛ Preventive Medicine Department
SUMMARY. An
analysis was made of the 119 patients treated for burns between 1 January 1996 and 31
October 1997 in our department. We considered the burned body surface area (BSA), depth of
burn, localization, mechanism of burn, place of accident, age, and sex. Children and the
elderly were the groups with the greatest risk of suffering burns. Lesions by liquids
constituted 60% of the cases. The average BSA was 20%. Dermal burns were involved in 74.8%
of the cases, the most common localization being the upper extremity (44%). At all ages
the highest prevalence was that of burns in the home, especially among children and the
elderly. The different rates between men and women who suffered burns in the home were
statistically significant (p < 0.001). Burns due to scalding liquids were the commonest
form in the home, with significant differences as regards other types of burn (p <
0.01). These data confirm that the home is the place most at risk for burns, especially in
children and the elderly, and that the domestic environment is the commonest site for
lesions due to scalding liquids.
Introduction
The home and the domestic environment
tend to be underrated as places where people are exposed to possible accidents. Generally,
the population intuitively considers the place of work and the roads to be the places that
present the greatest risk to physical integrity. If we consider statistics in our country,
Spain, we can see the large number of people affected by work-related accidents (almost
one million per year) and the high mortality due to traffic accidents (between four and
five thousand people die on the roads every year). Conversely, it is only relatively
recently that reliable data have been available with regard to accidents occurring in the
home and the domestic environment.
In the year 1981 the European Union resolved to establish a data-gathering system to
quantify and analyse the accidents and lesions that occur in the home. As a result of the
experience acquired from the functioning of this system, known as EHLASS (European Home
and Leisure Accident Surveillance System), it has proved its utility as a tool enabling EU
countries to define their policies as regards user protection in the field of safety.
Spain was incorporated into EHLASS in 1986. The last available EVILASS study in Spain,
dating back to 1995 and published in 1996, involved a minimum sample of 25,000 homes, in
which information was gathered regarding accidents that occurred in the home and its
surroundings. These data revealed that there were 986,598 casualties (almost the same
number as that in the work environment), which means that each year 2.5 persons per
hundred suffered this type of accident.
If the mechanisms causing accidents in the home and its environment are analysed, it can
be seen that almost 55% of the accidents were the result of a fall, either at the same or
at a different level, 29% were the result of a collision, crushing, or a cut, and 7% were
burns. If we restrict the area considered to inside the home, burns made up 15.7% of the
lesions. Despite the apparent low proportion of burns in the global perspective of
accidents, their effects on labour and their domestic and economic consequences for the
patients, plus the costs to the health care system, are such that they should be
considered to be a sociosanitary problem of the first order.
Many studies have shown the importance of the domestic environment as the main scenario
for the occurrence of burn accidents. All the studies, although referring to very
different countries as regards geographical location and socio-economic level, report that
the home is the most prevalent place for the occurrence of burn accidents. It is
interesting to note that the percentage of patients burned in the home in the USA and in
Turkey is similar (63% and 65% respectively) and that in both countries this location
occupies first place as regards the place where these lesions occur.' The data reviewed
show that the range of frequency of domestic accidents varies from 50 to 70%.
Generally speaking, the data presented here refer to patients seen in a hospital emergency
room. Patients initially attended at other levels of care and subsequently transferred for
treatment in hospital departments are thus not considered. The present study attempts to
analyse all burn cases seen in the Department of Plastic Surgery in the Air Force
University Hospital, in Madrid, regardless of how the patients arrived there.
Material and methods
An analysis was made of the burn
diagnoses of patients seen in the Department of Plastic Surgery in the Air Force
University Hospital (Madrid) between I January 1996 and 31 October 1997. The search
yielded 119 patients whose first two diagnostic digits were 94, according to the CIE9-MC
codes, i.e. a burn. The following lesion-related factors were analysed: burned body
surface area (BSA), depth of burn, anatomical location, causative mechanism, place of
accident, and age and sex of the patients (Table I). Of the 119 patients studied,
66 were male (55.5%) and 53 were female (44.5%). The average age was 40 yr.
| Burned body surface area
|
|
| Depth |
Epidermal (Ist degree)
Dermal (2nd degree)
Subdermal (3rd degree) |
| Anatomic location |
Head
Trunk
Upper extremity
Lower extremity |
| Mechanism |
| Hot liquid |
|
Explosion |
| Water |
|
Electricity |
| Flame |
|
Chemical |
| Hot solid |
|
Other |
|
| Place of accident |
Home
Work place
Other |
| Age (yr) |
| < 1 |
|
22-40 |
| 1-15 |
|
41-65 |
| 16-21 |
|
> 65 |
|
| Sex |
Male
Female |
|
Table 1 -
Variables analysed |
|
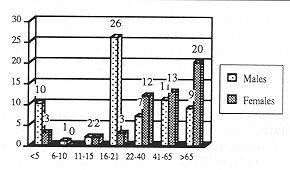
Grouping the patients by age groups, we
obtained the results presented in Fig. 1. These data show that the age groups of
early childhood and the elderly were those exposed to the highest risk of burn accidents.
Among children, those under the age of 5 yr presented the greatest incidence of this type
of accident.
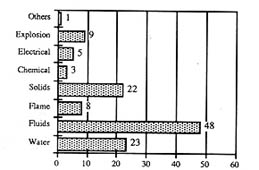
Analysing the data regarding the mechanism by which the burns were caused (Fig. 2), it
can be seen that lesions caused by liquids made up almost 60% of the total, onethird being
caused by water (scalding). The next most frequent mechanism, after liquids, was contact
with hot solids, which was more frequent than explosions, flame, chemical agents, and
electricity.
 |
 |
| Fig. 1 - Histogram of age distribution
frequencies. |
Fig. 2 - Distribution of burn mechanisms. |
|
With regard to the place
where the burn was caused it was found that in more than three-quarters of the cases
(76.5%) the burn occurred in the domestic environment (Fig. 3).
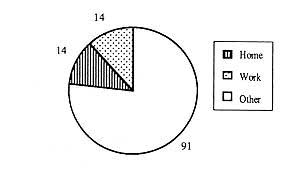 |
Fig. 3 - Distribution
by place where accident occurred. |
|
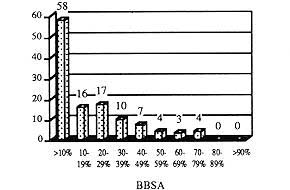
The burned body surface
areas of the patients making up the sample were grouped in ten intervals of ten points
each, on the basis of the CIE-9-MC classification. In nearly half of the 119 cases the
burns affected less than 10% BSA, and only I I patients had burns in more than 50% BSA. No
cases presented lesions in more than 80% BSA (Fig. 4). The average burned BSA
calculated from these grouped data was 20%.
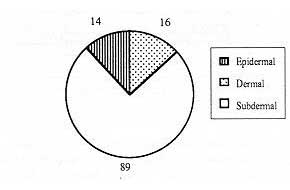
With regard to burn depth, the lesions were classified as epidermal, dermal, and
subdermal. When a patient presented coexisting lesions of different depths, the
classification was made as a function of the greatest depth. Applying these criteria, 16
patients had epidermal burns, 89 had dermal burns, and 14 had subdermal burns (Fig. 5).
 |
 |
| Fig. 4 -
Histogram of distribution of burned body surface area. |
Fig. 5 -
Pie chart of burn depth distribution. |
|
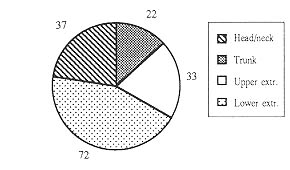
With regard to the body area affected, we
found that the anatomical locations burned most frequently were the upper extremities
(44%), followed by the lower extremities (22.5%) (Fig. 6). The overall total number
was higher than the number of patients enrolled because in many cases the lesions affected
more than one anatomical location. Classifying the burns of each anatomical location
according to depth, we obtained the findings shown in Fig. 7, which shows that the
commonest burns in all anatomical locations were dermal burns, with a percentage of well
over 50% in each area.
 |
 |
| Fig. 6 -
Distribution by place where accident occurred. |
Fig. 7 -
Frequency histogram of depth of burn according to anatomical location. |
|
When we associated the
patients age with the place where the accident occurred, also in relation to sex, we
obtained the results shown in Fig. 8.
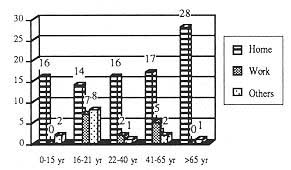 |
Fig. 8 - Frequency
histogram of place of accident as a function of age. |
|
This figure shows that in
all age groups the greatest prevalence of burns was found in the domestic environment.
This finding was especially significant in the age groups at either extreme: in infancy
(under 5 yr) 88.9% of the lesions were caused in the home, and in the elderly (over 65
yr), 96.5%. Similar results, but not as biased towards domestic lesions, were found in the
16-21 yr age group (48.3% of domestic burns), the 22-40 yr age group (84.2%), and the
41-65 yr age group (70.8%). When analysing the sex of the patients, we found that up to
the age of 21 yr males suffered more burns in all the locations studied. After this age
females were found to be at greater risk in the domestic environment than in other
environments, although the results were barely significant owing to the low number of
cases.
As regards only the sex and place of the accident, 88.7% of the females were burned in the
domestic environment (compared with 66.5% of the males). The percentage of males who
suffered an accident at work (15.1%) was double that of females (7.5%) (Table II).
| |
Home |
Work place |
Other |
Male
N=66 |
44
66.7% |
10
15.1% |
12
18.2% |
Female
N = 53 |
47
88.7% |
4
7.5% |
2
3.8% |
| |
S: p = < 0.001 |
AS: p < 0.1 |
S: p < 0.0 1 |
|
| Table
11 - Distribution of relation between sex and place of accident (S =
statistically significant difference, AS = almost significant difference) |
|
When comparing the data
obtained through a comparison of proportions, the differences between males and females
burned in the domestic environment were statistically significant (p < 0.001). The
comparison of data referring to the work place provided almost significant differences (1)
< 0.1). The difference in proportion of burns between males and females in other areas
was statistically significant (p < 0.01).
Considering the mechanism by which the lesion was caused as a function of sex, we obtained
the findings presented in Fig. 9. No statistically significant differences were
observed when comparing the sex in any of the mechanisms causing the lesions, with the
exception of electrical burns.
 |
Fig. 9 - Frequency
histogram of burn mechanisms as a function of sex (S = statistically significant
difference between proportions). |
|
Fig. 10 shows the
findings of the analysis of the place of the accident with reference to each of the
mechanisms causing the burn. In the majority of the mechanism groups, the preferential
place for the lesion to occur was the home. These findings provide statistically
significant differences when comparing the burns caused by hot liquids in the home with
those caused in the work place (p < 0.01). The proportional differences between burns
due to explosion in the work place and those occurring in other places are almost
significant (p < 0.01).
 |
Fig. 10 - Frequency histogram of percentages of burn mechanisms
and place of accident. |
|
Analysing the mechanism
causing the burn with regard to age group, we obtained the results presented in Fig.
11. These findings show that burns caused by hot liquids (including water) were
commonest in all age groups. Comparing the proportions of scald lesions in the different
age groups, we found significant differences in patients under 15 yr and aged 16-21 yr (p
< 0.05), and in those over 65 yr of age (p < 0.05). When the mechanisms involved
some other hot liquid, the differences were only almost significant when comparing
patients of less than 15 yr with those aged 16-21 yr (p < 0. 1). In burns caused by
flame or by chemical and electrical agents, there were no significant differences between
the age groups. However, there were significant differences between the proportions of
burns caused by hot solids when comparing the 15 and 21 yr age groups with the 41 and 65
yr age groups (p < 0.05) and that of the 15- and 21 -yr-olds with those over 65 yr (p
< 0.05). Finally, when comparing the proportion of burns due to explosion in the
different age groups, we found significant differences only between the groups of patients
younger than 15 yr and that aged between 22 and 40 yr (p < 0.01).
 |
Fig. 11 -
Percentile distribution of different burn mechanisms in different age groups. |
|
Discussion
Our results are consistent with those in
most of the reviews analysed, in the sense that they confirm that the domestic environment
is the main scenario where burn accidents occur. As said, the percentage of domestic burn
varies between 60 and 70% in the studies considered. With regard to our own country,
Spain, the studies published confirm that most of the burns seen in hospital were caused
in the home. One of the most representative studies is that conducted at the La Fe
Hospital Burn Unit in Valencia, which refers to 152 patients seen during 1992.' Of these,
61% suffered their burns in the home compared with 16% who were burned in road accidents
and 13% at work. Our results are even more significant with regard to the predominance of
domestic burns (76.5%) compared with those in other areas (Fig. 3). One of the
reasons for these numbers is the easy access to the plastic surgery out-patients
department available to patients seen in our hospital. Our department saw many of the
cases from the very beginning, while in other places some of the patients were seen first
at the level of a health care centre.
Comparing the data referring to domestic burns in different age groups (Fig. 8), we
found significant differences in patients in the 41-65 yr age group and in patents over 65
yr old age (p < 0.001). These results are especially influenced by the fact patients
aged 41-65 yr are actively employed. This consideration also explains the statistically
significant difference (p < 0.05) between patients under 15 yr and those over 65. Also,
the greater amount of free-time activities among young persons aged 16-21 yr would explain
the significantly lower percentage of domestic burns in this group compared with the
percentage of such burns suffered by those younger than 15 yr (p < 0.05).
Grouping the domestic burns case by sex and age (Fig. 8), we obtained interesting
findings in most of the age groups, with the greatest incidence in the youngest and oldest
patient age groups. These data are consistent with those reported in the last EHLASS study
and also with those obtained at La Fe Hospital in Valencia, where more than 80% of the
patients under 10 yr of age and older than 60 yr were burned in the home.
If there is any one place in the home that is at high risk, especially for children, it is
the kitchen. A series of circumstances come together in the kitchen that make it
especially liable to be the place for burn accidents. Mothers spend many hours in this
part of the house, and in small houses the youngest children are there with her. This is
especially significant in rural and low social class urban environments. In addition a
number of potential burn causes accumulate in the kitchen: burners (flame or electric),
oven, iron, kitchen utensils, small electrical appliances, recently cooked food, etc.
Although electrical appliances, large and small, may cause electrical burns in children,
the young most often suffer burns owing to the action of hot liquids that are spilled
owing to acts of imprudence on the part of adults and/or to the children's curiosity.
Despite the fact the domestic safety industry is continuously developing new devices to
prevent electrical risks among children, burns caused by this power source are still very
common, especially in the hands and mouth, due to contact between these areas and a source
of electricity. Among our cases, 5.5% of the burns in patients under 15 yr were electrical
in origin, caused by careless handling of elements by adults.
The elderly are the second most exposed population group at risk for domestic burns. Among
our cases, nearly all the elderly patients (96.5%) sustained their burns in the home. This
finding is consistent with the analysis carried out in the Wessex Burn Unit in the United
Kingdom over the period 1983-91. Of the 2,343 patients treated, only 5% were elderly, but
of these 98% were burned in the horne.` The commonest burn mechanisms were scalding and
contact with hot solids. In our review the commonest mechanisms causing burns were contact
with hot liquids (44.8%) and scalding (27.6%). The elderly presented the most complex burn
mechanisms. Thus it was not a rare event to have to attend an elderly patient severely
burned by the action of the flames of a burning tablecloth on a round table with a
catalytic burner too close to the cloth. Elderly people also sometimes attempt to combat
the cold by means of the joint action of a catalytic butane stove and an electrical stove,
both placed too close. If they fall asleep and a draught of air blows out the flame of the
catalytic stove, the butane emitted causes them to lose consciousness and fall over onto
the stove, where they may remain for a prolonged period of time. The severity of such
burns, especially with regard to depth, is very significant.
It is also significant that while in the younger age groups (under 15 yr of age) 75% of
the domestic burns were seen in males, in patients over 65 yr of age 71.4% were females.
If in the first case the results can be attributed to chance, in the second case they may
be related to the fact that women are more involved in potentially dangerous household
chores, especially while cooking. Women suffer the consequences of an accumulation of
hazardous elements in the kitchen: 34% of lesions caused in the home environment occur in
the kitchen, well ahead of those caused in the dining-room (12.6%), in the bedroom (4.6%),
or on the stairs (4%).' The pouring of hot oil from fryingpans or deep fryers and the use
of various other cooking utensils and kitchen accessories are the cause of 31% of burns
caused in the home. A relatively frequent mechanism is the "explosion" of a
pressure-cooker being opened. This is usually due to obstruction of the valve caused by an
accumulation of the detergents used to clean it. These burns are frequently spectacular,
causing great panic and sometimes traumatic contusion lesions as a result of the lid
hitting the victim's body.
it is surprising that at the ages when there is the greatest incidence of work activity
outside the home, i.e. 22 to 65 yr, the data do not show any significant numbers inclined
towards either sex. However, if all the patients are considered globally, regardless of
age, a greater incidence of work-related burns was found in men (Table II). The
highest numbers of burns occurring in other places appear in the 16- to 21-yr-olds
(27.6%). This result is probably related to the greater number of "fun"
activities typical of this age group. In this group four burns were caused by the exhaust
pipe of a motorcycle and three were the result of the explosion of firecrackers. The
remaining case was a burn in both lower extremities caused by an ultraviolet lamp with a
defective filter.
Fig. 11 relates the mechanisms causing burns to age. The findings show that hot
liquids (including water) were the commonest mechanism in infancy, with significant
differences when compared with older patients (p < 0.05) in the 16-21 yr age group. The
cause was generally carelessness on the part of the person in charge of the children. At
these ages the commonest cause of burns is hot liquids, generally water (i.e. scalding).
In 1986 the British administrative authority carried out an inspection of hot water taps
in homes. The result was that in 50% of the taps analysed the temperature of the water
coming out was over 60 'C.'' Although systems have been designed to control the
temperature of tap water, they are frequently not used. As a consequence scalding in
children is still very common and may occasionally be very severe because of the large
amount of BSA burned. Fig. 11 also shows that in the 16-21 yr age group the
commonest mechanism was contact with hot solids. This mechanism was significantly more
frequent in this particular age group than in the 41~65 yr group (p < 0.05) and in the
over-65 yr age group (p < 0.05). As we have said, at these ages we saw a high number of
cases of burns caused by contact with the exhaust pipe of motorcycles. The severity of
such burns is usually underrated by the persons involved, who continue to live their
normal life until after a few days they seek medical attention when the pain increases and
they realize that the lesion is important. By this time the burn, which initially may not
have been very deep, has become a deep dermal or subdermal lesion that requires surgical
treatment.
It is also significant that in this same age group (1621 yr old) the percentage burns
caused by explosions was as high as 15.8%. This figure is not surprising if we consider
that this is the age at greatest risk for accidents caused by the explosion of
firecrackers, fireworks, etc.
In our study, burns by flame (6.7% of the total number) were found with equal frequency
(37.5%) in the home environment and in other environments (i.e. environments that were
neither the home nor the work place) (Fig. 10). The finding that there were no significant
differences in favour of the home as the place where flame burns occurred is probably due
to the fact that the population attended was mainly urban. This is because in rural
environments or in small towns one of the main causes of thermal accidents is the use of a
low fire for both cooking and heating. This is frequently the cause of severe burns,
generally caused by the direct action of flame. One of the commonest causes of thermal
injury due to a low fire is an attempt to stir up a fire by throwing alcohol (i.e.
surgical spirit) onto it. The large flames that flare up when the alcohol ignites spread
from the fire to the container of the alcohol, causing ignition of the clothes and deep
extensive burns. This burn mechanism is common not only in rural environments but also in
barbecues and fireplaces in chalets. Thermal lesions caused by the ignition of flammable
liquids are also a very important burn mechanism in adolescents in the urban environment,
as a result of careless handling of such materials in games.
Electrical burns were not very frequent in the group studied (4.2%) and were usually due
to imprudence in the home. Indeed, all the electrical burns observed in our study occurred
in the patient's home. Many ordinary everyday situations can be dangerous in this regard.
Shaving, one of the first actions in a man's morning, can be the cause of serious
electrocution, simply by an attempt to pick up an electric shaver that has fallen into a
washbasin containing water. We have treated burns to the fingers caused by a man grasping
the cable of a shaver connected to the mains when trying to plug the shaver in. It is not
unusual for men to leave the cable plugged in all day and to connect the shaver to it
whenever it has to be used. Such burns are sometimes deep enough to leave sequelae in the
sensitivity of the fingertips. The widespread use of extension cords causes frequent burns
when, for example, a person grasps the free end when the other end is plugged in.
"Home-made" extension cords should never in fact be used at all - they should be
replaced by proper connection boxes with one or more, outlets and a cable to the mains. In
the group of accidents caused by electricity, home-made connections constitute one of the
commonest causes. When adhesive material is heated, it may ignite, with the result that it
loses its insulating characteristics and any contact with the skin may cause burns. This
is especially true with regard to small electrical appliances such as irons, blenders,
etc.
In the present study there were only three cases of chemical burns (2.5%). It is
surprising that none of these was found in children, considering the high risk of such
burns due to the storage of caustic products in the home. One lesion was caused by
extravasation of chemotherapy in a day hospital.
The disabled, whether physically or mentally, are a high-risk group for burns in their
normal living environment, i.e. the home. Individuals afflicted with a neurological or
psychiatric disease are especially at risk for burns in the home environment. Our review
yielded seven patients (5.9%) with a neuropsychiatric disorder (four epileptics, two
paraplegics, and one with severe mental retardation), all of whom were burned in the home.
These findings are similar to those of a review carried out in the Toronto Burn Unit in
Canada. 12 Of the 800 patients seen, 5% were neurological or psychiatric patients, 84% of
whom suffered their lesions at home. As also in elderly patients, the mechanism causing
the burn in such patients may be unsuspected. For example, the wheels of a wheelchair may
be dangerous if certain precautions are not taken. In one paraplegic patient with no
sensitivity in the lower extremities, a heat source was placed too close to the sides of
the wheelchair. This heated the metallic side-panel and caused severe subdermal burns to
the thighs. Such lesions are usually very deep and their treatment is severely impaired by
the patients' neurotrophic alterations.
RESUME. Les
Auteurs ont analysé 119 patients brűlés hospitalisés dans dans leur unité des
brűlures pendant la période 1 janvier 1996-31 octobre 1997. Ils ont considéré la
surface corporelle brűlée (SCB), la profondité des brűlures, la localisation, le
mécanisme de l'accident, le lieu, l'âge et le sexe. Les groupes des patients les plus
exposés au risque de brűlures étaient les enfants et les personnes âgées. Les
lésions causées Par les liquides constituaient 60% de tous les cas. La SCB moyenne
était 20%; 74,8% des patients ont subi des brűlures dermales, et l'extrémité
supérieure était la localisation la plus commune (44%). Pour tous les âges, les
brűlures les plus fréquentes se produisaient dans la maison, particuličrement pour ce
qui concerne les enfants et les personnes âgées. Les différences entre les patients
mâles et femelles atteints de brűlures dans l'environnement domestique était
statistiquement significatives (p < 0,001) Les brűlures causées par les liquides
chauds étaient les plus communes dans la maison, avec des différences significatives par
rapport aux autres types (p < 0,01). Ces résultats confirment que la maison est le
lieu le plus exposé au risque des brűlures, particuličrement pour les enfants et les
personnes âgées; en outre l'environnement domestique est le plus exposé au risque des
lésions causées par les liquides bouillantes.
BIBLIOGRAPHY
Sisterna Comunitario de Informaci6n sobre
Accidentes en cl Hogar y del Tiempo Libre. Informe Anual Espafla 1995. Ministerio de
Sanidad y Consumo, Madrid, 1996.
Haberal M., Ugar N., Bilgin N.: Epidemiological survey of burns treated in
Ankara, Turkey and desirable burn-prevention strategies. Burns, 21: 601-6, 1993.
Fadaak K, Fawzy S., EI-Fayomy S. et al.: Admission and pattern of burn injuries at a new
Burn Unit at Unayzah, Qassim, Saudi Arabia. Ann. Burns and Fire Disasters, 9: 73-8, 1996.
Belba G., Andrea A., Danti J. et al.: Some epidemiological data regarding burn
patients treated during 1992 in Albania. Ann. Medit. Burns Club, 7: 5-7, 1994.
Dayoub A.: Les brűlures dans la vie domestique ŕ Alep, Syrie. Ann. Medit. Burns
Club, 1: 17-19, 1988.
Duggan D., Quine S.: Burn injuries and characteristics of burn patients in New
South Wales, Australia. Burns, 2: 83-8, 1995.
Jayaraman V., Mathangi K., Davies M.R.: Burns in
Madras, India: An analysis of 1368 patients in one year. Burns, 19: 339-44, 1993.
Lochaitis A., Ifiopoulou E., Kommakis E. et al.: Burns as a result of domestic
accidents and their prevention. Burns, 18: 416-8, 1992.
Serna C., Terren J., Pons S. et al.: Epidemiological analysis of patients
admitted to the burns centre in Valencia during the year 1992. Ann. Medit. Burns Club, 6:
224-8, 1993.
Sarhadi N., Kincaid R., McGregor J., Watson J.:
Burns in the elderly in the South East of Scotland: Review of 176 patients treated in the
Bangour Burns Unit (1982-91). Burns, 21: 91-5, 1995.
Stephen F.R., Murray J.P.: The prevention of hot tap water burns - a study of
electric immersion heater safety. Burns, 17: 417-22, 1991.
Backstein R., Peters W., Neligan R: Burns in the
disabled. Burns, 19: 192-7, 1993.
This paper was received on 10 April 1999.
Address correspondence to: Dr Fco. Xavier Santos
Heredero, Plastic Surgery Department, Hospital Universitario
del Aire, Cl Arturo Soria 82, 28027 Madrid, Spain.
Tel.: 91 407 5900; e-mail: xsantos@haire.es |
BRITISH BURN ASSOCIATION
The 1999 Laing Memorial Essay
The Executive Committee of the British
Burn Association invites submissions for the 1999 prize essay. The chosen title is:
"Burns Survivors
and their Rehabilitation"
The essay submitted (3 copies) should
be of length 5000-7000 words maximum and in the style used by BURNS Journal. Award of the
prize (Ł500) will be made on the judgement of two referees appointed by the BBA. A
prizewinning essay will be eligible for publication in BURNS at the discretion of the
editor.
Entries should be submitted to Mr Ken Dunn, Secretary to the BBA, The Burns Unit,
Withington Hospital, Manchester M20 8LR, UK; closing date 31 December 1999. |
|