Annals of
Burns and Fire Disasters - vol. XII - n° 3 - September 1999
ANTIBIOTIC SALICYLATE VASELINE: A TOPICAL TREATMENT OF CHOICE IN BURNED
DIABETIC PATIENTS?
Napoli B, D'Arpa N, laia A,
Sferrazza G, Masellis M.
Divisione di Chirurgia Plastica e Terapia delle Ustioni,
Ospedale Civico, Palermo, Italy
SUMMARY. The healing of burns in
diabetic patients is delayed by the vascular obstruction due to the disease and by the
effects of diabetes (insufficient inflammatory response, insulin insufficiency and/or
resistance). Local treatment is thus of fundamental importance for the healing of the
wounds and for metabolic compensation, which is closely related to healing and which in
turn it affects. In their clinical practice, the authors of this paper use antibiotic
salicylate vaseline as their elected topical treatment of burns in diabetic patients in
the light of the fact that antibiotic salicylate vaseline has a keratolytic and
antimicrobial effect, improves local circulation, and increases the activity of insulin.
Introduction
Various researchers in the past have proposed
the use of salicylate vaseline with various concentrations of salicylic acid and of
antibiotic antiseptic salicylate vaseline (AASV) in the local treatment of burns.
In patients with localized burns in particular body areas (face, neck, flexor folds,
perineal area), in whom surgical escharectomy is difficult to perform, or in bad physical
condition (serious damage to upper airways, serious shock, previously generally poor
physical condition, etc.), in whom early escharectomy would be dangerous both
aesthetically and quoad vitam, the use of the proposed method permits good and
rapid chemical escharectomy, without blood loss. It also improves the prospects of good
skin-graft take.
Antiseptics and antibiotics were added to the salicylate vaseline in order to increase
salicylic acid's antimicrobial effect.
It happens ever more increasingly that Burn patients are unaware of their diabetic
condition, which therefore went untreated. This and other physiopathological and clinical
considerations regarding diabetes prompted us to study more deeply this method's possible
local and more general effects on diabetes. We were also interested in its influence on
the healing of the damaged areas.
It is well known that wounds in diabetic patients are extremely slow-healing. This delay
is due to the combination of two factors:
- disturbances in local blood circulation
- the effects of hyperglycaernia (insulin insufficiency or
resistance)
The circulation disorders are a consequence of
the vascular obstructive disease. This affects above all the peripheral vessels, with
negative consequences for oxygen flow (hypoxia) and for the nutritional substances
reaching the wounds (malnutrition).
The inflammatory response in diabetic patients is insufficient, and the consequences of
insulin deficiency (blockage of anaerobic glycolysis, from which the white blood cells
receive most of their energy) are associated with those of hyperglycaemia. This condition
inhibits phagocytosis and therefore the intracellular lysis of bacteria ingested by wound
macrophages. This is why diabetics are so liable to infection.
Another important factor involved in the slow healing of diabetic patients' wounds is the
direct effects of insulin deficiency on the fibroblasts as regards glucose absorption and
protein synthesis, both of which are considerably reduced.
Material and methods
The AASV used was prepared following the same
criteria as that for non-diabetic individuals, i.e. on the basis of the findings of the
antibiograrns performed on germs isolated from burn wounds in patients admitted in periods
just before admission of these patients, until it becomes necessary to select patients on
the basis of the sensitivity of the particular infecting germ isolated from the patients.
The same applies to the choice of salicylic acid concentration (type of Burn, dry or wet,
site, approximate estimate of degree).` It must not however be forgotten that in diabetic
patients higher concentrations are more likely to lead to hypoglycaernia. The Burns
treated were either partial- or full-thickness, in diabetics who were already on insulin
treatment or began treatment after coming to us. Six patients (4 male, 2 female) were
observed (age range 38-65 yr). The following parameters were assessed in each patient:
time for elimination of eschar after initiation of treatment, amount of graft take,
glycaemia monitoring, and the effect of treatment on the healing of untreated superficial
burns.
Case histories
P.V., male, age 48 yr, admitted 5 June 1995
with partial- and fullthickness electric and flame burns, 30% BSA. Diabetes, of which the
patient was unaware, was diagnosed after hospitalization. This required the administration
of insulin. For local treatment we used AASV. The patient received a free skin graft on
22/6/95 in order to cover the residual burn areas, which were less than 5% BSA (Fig. 1).
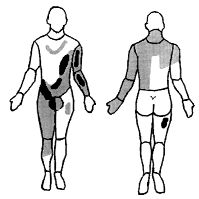 |
Fig. 1 - Burns distribution: operated
areas indicated in black. |
|
N.G., male, age 62 yr, admitted 2 September
1995 suffering from previously unsuspected diabetes. Presented sustained partial- and
full-thickness flame burns in about 20% BSA. Third-degree circumferential Burns in left
leg and thigh. Burns subjected to surgery on 18/9/95 after surgical escharectomy. On
28/9/95 there was no sign of infection and the grafts had taken perfectly.
A.G., male, age 59 yr. Patient unaware of
preexisting disease. Suffering from partial- and full-thickness flame Burns in 20% BSA.
Admitted 13 September 1995. Insulin therapy initiated after a few days, together with
local treatment with AASV. The patient was subjected to skin grafting on 29/9/95 for the
3% residual burns that had not yet healed.
L.F., female, age 50 yr, suffering from
flame burns in upper left limb. Admitted 9 October 1995. This diabetic patient was
discharged completely cured on 31/10/95. The formation of good uninfected granulation
tissue during the second week of local treatment with AASV was followed in the third week
by total recovery. Demarcation and chemical escharectomy of necrotic tissue was performed
in the first week.
C.G., female, age 57 yr, diabetic, admitted
16 January 1998 following explosion of gas cylinder. Partialthickness Burns in 65% BSA.
Treated with salicylic vaseline. Deeper areas surgically cleansed on 28/01/98. This
patient had a severe cardiopathic condition and died from cardiological complications on
5/2/98, when she had almost recovered from her local injuries.
S.M., male, age 38 yr, admitted 15 November
1998 for partial- and full-thickness flame burns in 10% BSA. Discharged fully recovered on
7/12/98. Also in this case monitoring of the deepest wounds showed that they healed in
three weeks without any infective complications (Figs. 2-5).

|
|

|
| Fig. 2 -
Partial-thickness burn and entire anterior thorax and neck. |
|
Fig.
3 - Same case. Partial -thickness burn and entire posterior thorax and neck. |

|
|

|
Fig.
4 - Same case. Healing after three weeks' treatment with antibiotic salicylate
vaseline. |
|
Fig. 5 - Same case. Healing after three weeks'
treatment with antibiotic salicylate vaseline. |
|
Discussion
Diabetes is a widespread disease. Those
afflicted are however often unaware of their disease, which is not easy to manage,
especially if complicated by burns.
The slow healing of the lesions is due to various mechanisms related to the basic diabetic
condition and especially to the ease with which microbial infections affect diabetic
patients. This delay has direct effects on the possibility of metabolic compensation.
The local treatment of burn wounds in diabetic patients is therefore of primary
importance, not only as regards the healing of the burns but also as regards control of
the diabetic condition. If the local treatment of burns in diabetic patients is to be
effective, it is therefore necessary that it should influence the mechanisms that delay
healing. Salicylate vaseline appears to possess these qualities.
Routine therapeutic doses of salicylates do not exert any important direct action on the
cardiovascular system. High doses, however, cause the dilatation of peripheral vessels
owing to the direct effect on the smooth musculature;' in diabetic patients they could
therefore improve local circulation local circulation. By potentiating insulin and
reducing its consumption, salicylates may be able to produce an excess of insulin at the
level of the lesion. This would reduce glycaernia, improve the inflammatory response, and
improve fibroblast activity.
For these reasons the use of salicylate vaseline would appear to considerably stimulate
the formation of uninfected granulation tissue and subsequent reepithelialization. This
occurs because its keratolytic and antimicrobial action would appear to be associated with
the improved local circulation and the increase in insulin activity.
Conclusions
Even if the number of cases we treated was
limited, our results enable us to hypothesize that antibiotic salicylate vaseline may be
useful in the topical treatment of diabetic burn patients. In addition to its keratolytic
and antimicrobial action, it influences the mechanisms that delay wound healing in
diabetic patients. When used in the local treatment of lesions in diabetic patients,
antibiotic salicylate vaseline promotes:
- the healing of partial-thickness burns;
- the healing of full-thickness burns of
limited extent;
- the reduction of the extent of widespread
partialand full-thickness burns.
RESUME. La guérison des brűlures dans les
personnes atteintes de diabčte est retardée soit par la maladie vasculaire obstructive
soit par les effets du diabčte (réponse inflammatoire insuffisante, insuffisance et/ou
résistance de l'insuline). Le traitement local devient conséquemment d'importance
fondamentale soit pour la guérison soit pour ce qui concerne la compensation
métabolique, étroitement liée ŕ cette guérison, et qui, ŕ son tour, agit sur elle.
La pratique clinique a porté les Auteurs ŕ utiliser la vaseline salicylée antibiotique
parce que, ŕ part son action kératolytique et antimicrobienne, elle améliore la
circulation locale et intensifie l'activité de l'insuline.
BIBLIOGRAPHY
Maviglio P., Mavilio D., De
Donno G., Fiume D.: The use of salicylate vaseline in the debridement of burns. Ann. Burns
and Fire Disasters, 3: 75-8, 1990.
Masellis M.: Association of
salicylic vaseline with antiseptics or antibiotics in topical treatment of burns.
"Care of the Burn Wound", May, Dogo (eds.), Int. Congr. Geneva, Karger,
Basel, 1- 6, 1985.
Masellis M., Vitale R., laia A.: Surgical and
chemical necrectomy: Two methods for debridement of the burn wound. Comparative analysis.
Riv. Ital. Chir. Plast., 13: 17-22, 1981.
Sferrazza G., D'Arpa N., laia A., Napoli B.,
Masellis M.: Escarectomia chimica con vaselina salicilata. Conferma di una metodica.
Proceedings 47th SICPRE Congress, Palermo, September 1998.
Goodson W.H., Radolf J., Hunt T.K.: Guarigione
delle ferite e diabete. In: "Ferite cicatrizzanti e ferite
infette", Hunt T.K., Liviana editrice, Padua, 1983.
Napoli B., D'Arpa N., Masellis M.: Diabetes and burns - Problems of diagnosis and therapy. Ann. Burns and Fire
Disasters, 9: 131-4, 1998.
Goodman and Gilman, "Le basi farmacologiche
della terapia". Editoriale Grasso, Bologna, 1982.
Paroli E.: "Farmacologia clinica.
Tossicologia". Societŕ Editrice Universo, Rome, 1985
This paper was
received on 30 March 1999.Address correspondence to:
Dr B. Napoli
Divisione di Chirurgia Plastica e Terapia delle Ustioni - Ospedale Civico
Via C. Lazzaro
90127 Palermo, Italy |
|