Annals of
Burns and Fire Disasters - vol. XII - n° 3 - September 1999
SUBESCHAR INFILTRATION OF EPINEPHRINE PRIOR TO EARLY EXCISION OF BURN
WOUNDS - TECHNICAL REFINEMENTS
Janezic T.
Burns Unit, Ljubljana Clinical Centre, Ljubljana, Slovenia
SUMMARY. The early excision of burn wounds may lead to
massive blood loss, which often becomes a major factor limiting the excision area. In
order to diminish intra-operative blood loss following early excision of burn wounds,
epinephrine solution may be injected under the burn eschar prior to excision. At the Burns
Unit in Ljubljana (Slovenia) the technique of subeschar infiltration of epinephrine
solution was started in 1988. Up to now the technique has been used in more than 500
patients. During the last ten years of clinical experience with this technique, several
important technical details have been found to be important. The most important points of
this technique are anaesthesia, the concentration of epinephrine hydrochloride, marking of
the area to be inoltrated, the instruments used, the plane of infiltration, the time
interval between infiltration and excision, assessment of the burned tissue to be excised,
the volume of epinephrine solution injected, and haemostasis.
All these factors are described and discussed in this report.
Introduction
Excision in the first five days post-injury
has been widely accepted as the method of choice in the treatment of full-thickness burn
wounds. Early excision produces massive blood loss' which often becomes a major factor
that limits the area of excision, thus greatly influencing the survival and the morbidity
of burned patients. Many methods of reducing intra-operative blood loss have been
described: use of the tourniquet for excision on the extremities' application of a topical
solution of epinephrine hydrochloride, infusion of I -desamino-8-D-arginine vasopressin,
intravenous application of triglycyl-lysine-vasopressin, early burn wound excision (first
24 h post-burn), and subeschar infiltration of vasoconstrictors such as ornithine 8
vasopressin (POR 8) or epinephrine hydrochloride.
The technique of subeschar infiltration with epinephrine solution in areas where a
tourniquet could not be applied was first used at the Ljubljana Department of Plastic
Surgery and Burns in 1988. Since then the technique of subeschar infiltration with
epinephrine solution prior to excision of burn wounds has been used in more than 500
burned patients. Several technical details have been found to be important if the
technique's maximum effect is to be achieved.
Method and technique
Anaesthesia
The anaesthetist needs to know the quantity and concentration of epinephrine solution
injected. When epinephrine is injected beneath the burn eschar, certain anaesthetic drugs,
e.g. halothane, should be avoided. The type of anaesthesia should be carefully chosen.
Even when large quantities of epinephrine are injected (i.e. more than 0.03 mg/kg) there
have been no reports of major complications due to epinephrine's systemic effects. Some
minor cardiovascular effects of injected epinephrine were occasionally observed but these
did not require therapeutic measures. Mild metabolic acidosis was experienced by several
patients but this had ceased by the end of the surgical procedure.
Concentration of epinephrine
hydrochloride
The epinephrine solution used at the Burns Unit in Ljubljana is composed of 500 ml
normal saline, with an added I ml 1/1000 aqueous epinephrine hydrochloride (I mg
epinephrine hydrochloride/500 ml solution , 1:500 000). On the basis of my experience this
concentration of epinephrine represents the optimurn ratio between the weakest
concentration of epinephrine and its effect.
Marking of the infiltration area
It often happens that the areas to be infiltrated are extensive, with the result that
the surgeon may fail to inject some areas or even inject some twice. In order to inject
the epinephrine solution evenly under the whole burn area, the eschar should be marked
with transversal lines, using an ordinary surgical marker, dividing the area into small
4-cm-square rectangles. By injecting the epinephrine solution successively into each
rectangle, the volume of epinephrine solution per unit area injected is distributed much
more evenly (Fig. 1).
 |
Fig. 1 - Marking the
eschar prior to infiltration. |
|
Infiltration instruments
Large quantities of epinephrine solution can be injected manually, using syringes and
needles. There are also commercially available pumps on the market. In our department we
use a device assembled from parts commonly found in any intensive care unit. The needles
used are of standard 0.8 mrn thickness and should be at least 8 cm long if extensive areas
to be infiltrated.
Depth or plane of infiltration
The infiltration of the epinephrine solution should be performed in the same plane as
the planned excision of the burned necrotic tissue. The depth of infiltration is of utmost
importance in order to achieve the maximum vasoconstriction effect in the desired plane of
excision and thus to minimize surgical blood loss. The depth of the excision and thus the
plane of the epinephrine infiltration are judged on clinical grounds. The results of the
eschar biopsy taken for the quantitative bacteriological culture help to determine the
depth of the burn and subsequently the plane of the epinephrine infiltration (Fig. 2).
 |
Fig. 2 - Biopsy of the
burn eschar for determination of burn depth. |
|
Time interval between
infiltration and excision
The time interval between infiltration of the epinephrine solution and excision of
burned tissue is very important for epinephrine's optimal vasoconstricting effect. In my
experience the optimal time interval between injection and excision is 10-15 min. One can
also determine the ideal time to start the excision by clinical observation of the healthy
skin adjacent to the burned eschar. Blanching of the area (0.5 to I cm wide) of the
healthy skin adjacent to the burned eschar is a sign that epinephrine's vasoconstricting
effect has taken place (Fig. 3).
 |
Fig. 3 - Blanching of
adjacent healthy skin. |
|
Assessment of viable and
nonviable tissues during excision
With the epinephrine infiltration technique, it is not possible during excision of the
burn eschar to assess viable and nonviable tissues by the classic signs of tissue
bleeding, owing to vasoconstriction. The viability of the tissues should be judged by the
appearance of the tissues, which is similar to that seen when performing an excision under
a tourniquet. Viable dermis is pearly-white in appearance, moist, and devoid of thrombosed
vessels. Healthy subcutaneous fat is shiny and yellow colour and also devoid of thrombosed
vessels (Fig. 4).
The minor haernatomas occurring in the course of the epinephrine injections should be
carefully considered and not be mistaken for necrotic tissues (Fig. 5).
 |
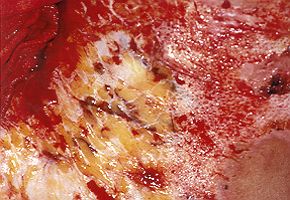 |
| Fig. 4 - Appearance of
healthy tissue on injection of epinephrine, |
Fig. 5 - Haernatorna in
the course of a previous epinephrine injection. |
|
Volume of'epinephrine
solution per unit of area injected
The median volume of epinephrine solution injected is about 0.7 to I ml per kg of body
weight per 1% debridement. This means that a 70-kg patient would receive 50 to 70 ml of
epinephrine solution under each 1% of body surface debrided. Some adult patients therefore
received up to 1500 ml of epinephrine solution.
Accurate haemostasis
Haemostasis is performed by bipolar electrocoagulation in small vessels and by
ligatures in larger ones. The bleeding of the cut vessels, especially of small arteries in
the debridement area, is greatly diminished owing to epinephrine's vasoconstrictor effect.
This may mislead the surgeon into not coagulating the smallest bleeding points, with the
risk of early post-operative bleeding. When using the epinephrine infiltration technique
one must therefore be careful to perform very thorough haemostasis.
Discussion
The early excision of burn wounds may produce
brisk, massive bleeding from the excised area. The intra-operative blood loss resulting
from the excision of burned tissues often limits the area to be excised, with important
effects on the morbidity and mortality of critically ill patients with thermal injuries.
After the excision of smaller burn wounds, patients often need transfusions following
intra-operative blood loss. The reduction of intra-operative blood loss following early
excision of burn wounds therefore lessens morbidity and mortality in extensively burned
patients. Also, in patients with minor burn wounds, transfusion may often be avoided.
Several techniques to reduce intra-operative blood loss following the early excision of
burn wounds have been described. In our unit we use tourniquets for excisions on the
extremities. Epinephrine solution is used topically to reduce blood loss from donor sites.
To reduce blood loss from other areas, we have made considerable use over the past ten
years of the subeschar infiltration of epinephrine solution. When this technique was being
introduced in our unit the most important question was how much epinephrine could be
injected without causing any of epinephrine's systemic effects, namely cardiovascular
manifestations and metabolic acidosis. Gradually more and more epinephrine solution was
injected without any noticeable important systemic effects due to epinephrine. The
anaesthetist also gradually adapted the type of general anaesthesia. We now often inject
more than 1500 ml of the above-described epinephrine solution in adult patients without
any sign of systemic effects of epinephrine requiring additional therapeutic measures.
The second question regarding the technique of epinephrine infiltration is the rebound
phenomenon. It is my opinion that post-operative bleeding due to the vasodilatation of
vessels previously vasoconstricted by epinephrine is mainly caused by inadequate
intra-operative haemostasis.
The coagulation of the vasoconstricted vessels is performed on the basis of a different
clinical intra-operative assessment from that in the area where epinephrine was not used.
It is necessary to take into an account the changed appearance of the burn wound due to
vasoconstriction where the tissues look similar to those under tourniquet
Graft take did not differ from that in areas where epinephrine was not injected, and the
infection rate in excised burn wounds was not observed to be higher.
Subeschar injections of epinephrine solution may prolong the operative procedure by about
30 min if injected manually. Use of the injecting device substantially shortens injection
time.
Conclusion
To conclude, it can be said that, technically
speaking, the subeschar infiltration of epinephrine solution is very easy to learn and can
be used even by surgical residents with limited surgical experience.
RESUME. L'excision
précoce des brűlures peut causer des pertes massives de sang, ce qui peut devenir un
facteur important qui limite l'extension de la zone d'excision. Pour réduire les pertes
intraopératives de sang aprčs l'excision précoce des brűlures, il est possible
d'injecter une solution épinephrine dans l'escarre avant d'effectuer l'excision. A
l'Unité des Brűlures ŕ Ljubjlana (Slovénie) on utilise depuis 1988 la technique de
l'infiltration sous l'escarre d'une solution épinephrine. La technique a été employée
dans plus de 500 patients. Pendant ces dix années d'expérience clinique avec la
technique divers aspects techniques se sont révélés importants, dont les plus
significatifs sont l'anesthésie, la concentration de chlorure hydrique épinephrin,
l'indication de la zone destinée ŕ l'infiltration, les instruments, le plan
d'infiltration, l'interval entre l'infiltration et l*excision, l'évaluation du tissu
qu'il faut exciser, le volume de la solution épinephrine qu'il faut injecter, et
l'hémostase. Tous les aspects de la question sont décrits et commentés par l'Auteur.
BIBLIOGRAPHY
- Heimbach D.M.: Early burn wound excision and grafting. In:
Boswick J.A., It (ed.): "The Art and Science of Burn Care", Rockville, Aspen,
65-73, 1987.
- Janzekovic Z.: A new concept in the early excision and
immediate grafting of burns. J. Trauma, 10: 1103-8, 1970.
- Janzekovic Z.: The
burn wound
from the surgical point of view. J. Trauma, 15: 42-62, 1975.
Brcic A., Zdravic F.: Lessons leamt from 2409 burn patients operated by early excision. Scand. J. Plast. Surg.,
13: 107-9, 1979.
Brezel B.S., McGeever K.E., Stein J.M.: Epinephrine v thrombin for split-thickness donor
site hemostasis. J. Burn Care
Rehabil., 8: 132-4, 1987.
Housinger T.A., Hills J., Warden G.D.: Management of pediatric facial burns. J. Burn Care Rehabil., 15: 408-11, 1994.
Snelling C.F.T., Shaw K.: The effect of topical epinephrine
hydrochloride in saline on blood loss following tangential excision of burn wounds. Plast.
Reconstr. Surg., 72: 830-4, 1983.
Haith L.R., Jr, Patton M.L., Goldman W.T., McCutchan K.M.:
Diminishing blood loss during operation for burns. Surg. Gynaccol. Obstet., 176: 119-23,
1993.
Garner W.L., Thomson P.D., Moore N.P., Rodriguez J.L., Smith D.J., Jr.: Effect of
triglycyl-lysine-vasopressin on skin blood flow and blood loss during wound excision in
patients with burns. J. Burn Care
Rehabil., 14: 458-60, 1993.
Desai M.H., Herndon D.N., Broemeling L., Barrow R.E., Nichols
R.J., Rutan R.L.: Early burn wound excision significantly reduces blood loss. Ann. Surg.,
211: 753-9, 1990.
Clarke A.M., Solomon J.R., Keogh E.J.: The LISC of a new
vasoconstrictor in the management of burns. Med. J. Aust., 2: 361 - 362, 1972.
Janezic T., Prezelj B., Brcic A., Arnez Z., Zaletelj-Kragelj L.: Intraoperative blood
loss after tangential excision of burn
wounds treated by subeschar infiltration of epinephrine. Scand. J. Plast. Reconstr., 31:
245-50, 1997.
Hughes W.B., De Clement F.A., Hensell D.O.: Intradermal
injection of epinephrine to decrease blood loss during splitthickness skin grafting. J.
Burn Care Rehabil., 17: 243-5, 1996.
Janezic T.: Injector: A simple device to
inject large quantities of vasopressor anesthetic solutions. E. J. Plast. Surg., 22:
195-6, 1999.
This paper was received on 18 May 1999.
Address correspondence to:
Assistant Prof. Tomas Janezic, M.D., Head of the Burns Unit
Department of Plastic Surgery and Burns
Clinical Centre Ljubljana Zaloska 7
1525 Ljubljana, Slovenia
Tel.: +386 61 323 983 - fax: +386 61 316 889 |
|