Annals of
Burns and Fire Disasters - vol. XII - n° 3 - September 1999
ADIPOFASCIAL
TURN-OVER FLAP COMBINED WITH NERVE RECONSTRUCTION IN SEVERE INJURY OF THE ELBOW
Calcagni M., Liguori G.C., Bollero D., Clemente A., Risso
D., Stella M.
Department of Plastic Surgery and Burn Unit,
Traumatological and Orthopaedic Centre, Turin, Italy
SUMMARY. Severe injury of the elbow
involving nerves is quite common. Several techniques have been proposed for resurfacing
this region: distant pedicled flaps, muscle and musculocutaneous flaps, fasciocutancous
flaps, and free flaps. The appropriate indications for all these techniques are still
controversial. In recent years adipofascial tum-over flaps have been used. These can be
raised without sacrificing the overlying skin and tailored in thickness to fill different
defects. The flap is outlined on the flexor aspect of the arm. The subcutaneous layer is
exposed through an H-shaped incision, The skin is dissected at dermal level and the
subcutaneous tissue with the deep fascia is then elevated in the planned size. A
two-centimetre pedicle is left intact proximal to the defect and the flap is turned over
to fill it. Two cases treated with this technique are presented.
Introduction
Traurnas and burns can cause severe injury
to soft tissues of the elbow and are often complicated by nerve exposure and lesion.
Several techniques have been proposed for resurfacing this region: distant pedicled flaps,
muscle and musculocutaneous flaps, fasciocutaneous flaps, and free flaps. The appropriate
indications for all these techniques are still controversial. Distant flaps require
multiple stages and long immobilization periods leading to stiffness of secondary joints.'
Local muscle and musculocutaneous flaps use functional muscle from the arm and cause gross
distortion of the limb shape. Fasciocutaneous flaps are very useful and careful
indications can minimize morbidity of the donor site, but the cosmetic appearance of
grafted donor sites is poor; moreover, the dissection of pedicles is often tedious. Free
flaps provide excellent results, but in heavily traumatized limbs healthy recipient
vessels can be a major problem.
In recent years some important contributions have been made to the understanding of the
vascular anatomy of subcutaneous tissue . These findings have made it possible to create
new adipofascial flaps based on direct and reverse blood flow in both the upper and the
lower limbs, This paper describes applications of this type of flap in the elbow region
combined with nerve repair.
Materials and methods
Two patients underwent surgical procedures
for reconstruction of post-traumatic sequelae of the elbow region with involvement of deep
nerves, requiring neurolysis and/or grafting.
The patients were both male and aged 23 years. Followup was for two years.
Surgical technique
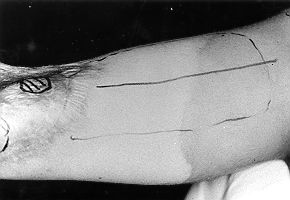
After debridement of the lesion a flap of adequate dimensions is marked on the flexor
aspect of the arm, over the biceps muscle (Fig. 1). The skin is incised in an H-shaped
pattern and an adequate undermining is carried out, leaving intact subcutaneous tissue
beneath (Fig. 2).
 |
 |
| Fig.
1 - Flap outlined on anterior aspect of arm over biceps muscle (all figures
relate to case 1). |
Fig. 2 -
Skin elevated, leaving intact subcutaneous tissue bencath. |
|
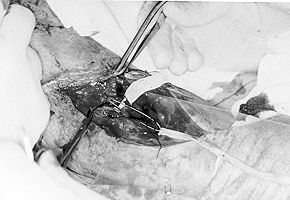
An adipofascial flap with a
distal pivot is then outlined and elevated from the underlying muscle (Fig. 3). Vascularization
occurs through perforators of the rete cubiti with the distal fascia of the biceps muscle,
as described by Marty. The flap is turned over to fill the defect and cover the nerve
repair. The exposed fascia is then grafted with split-thickness skin grafts. The donor
site is closed by approximation of the skin flaps over a suction drain.
 |
Fig. 3 -
Flap dissected free from muscle. Note brisk bleeding from distal edge of flap. |
|
Case reports
Case I
S.A., a 23-year-old steel worker, sustained a deep Burn of the flexor aspect of the elbow
region.
The patient was first admitted to a peripheral hospital and later transferred to our
department. The lesion was already infected and the eschar was firmly adherent. The
median-nerve innervated territory was hypaesthesic, while the u1nar and radial territories
showed no impairment. The median-nerve innervated intrinsic muscles were paralysed and the
u1nar muscles were normal. The epitrochlear muscles were hypopotonic.
The first procedure was surgical debridement carried down until the muscles were widely
exposed. The epitrochlear muscles were partially necrotic and were debrided together with
part of the biceps tendon. The median nerve was necrotic and was excised for 12 cm of its
length. The wound was covered with split-thickness meshed skin grafts.
The skin grafts were subsequently removed and the wound covered with a turn-over
adipofascial flap. In the same procedure the median nerve was isolated, the stumps were
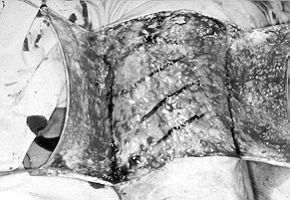
trimmed, and a silicone tube was sutured to the cut ends (Fig. 4). The exposed deep
surface of the fascia was then covered with split-thickness skin grafts (Fig. 5).
 |
 |
| Fig.
4 - After excision of the necrotic median nerve, trimming of stumps and suturing
of silicone tube to cut ends. Hand to the left. |
Fig.
5 - Fascia finally covered with split-thickness skin graft. |
|
One month later the
silicone tube was removed and the median nerve was reconstructed with a cable graft of
sural nerve pulled through the pseudo-sheath surrounding the silicone tube (Fig. 6).
At the same time the superficial flexor tendons of the ring and little fingers were
transferred for reanimation of index finger flexion and thumb anteposition (Fig. 7).
The patient is now doing
well. The elbow has a satisfactory range of motion, and the biceps muscle has good
strength! The median territory has satisfactory sensibility with a standing two-point
discrimination of 10-12 mm and a moving two-point discrimination of 8 turn.
Case 2
S.F., a 23-year-old student was referred to us six months after a car accident suffering
from a scar contracture of the elbow consequent to an exposed fracture (ulna, radial and
distal part of the humerus). The neurological examination showed clinical signs of u1nar
nerve neurotmesis and median nerve compression at the elbow, confirmed by EMG findings.
After scar excision, the u1nar nerve stumps were exposed and trimmed. The 7-cm long gap
was filled with a cable graft of sural nerve. The median nerve was heavily scarred, but no
neural damage was found. Thorough neurolysis was then performed. A turn-over adipolascial
flap of the arm fascia, 18 em long and 8 em wide, was sculptured and turned over on the
nerve graft. The exposed deep surface of the fascia was then covered with a
split-thickness skin graft. The patient is now doing well, the elbow has a good range of
motion, and protective sensibility has returned to the ring and little fingers.
Discussion
Various types of
flaps are available for resurfacing the elbow region. Among these the adipofascial
turn-over flap of the brachial fascia can be a good solution for reconstruction of severe
lesions of the elbow and proximal forearm soft tissues, especially when the main vascular
axis is impaired.
Pedicled flaps involve prolonged immobilization, while free flaps often require longer
operating times and suitable recipient vessels.
The u1nar fasciocutaneous flap is very reliable and its pivot point is in a favourable
position. However, a major blood vessel of the forearm has to be sacrificed, and it is
thus imperative that Allen's test be performed before the flap is raised.
A similar disadvantage is presented by the posterior interosseous flap, which is also
tedious to dissect. Moreover, the interosseous nerve sometimes crosses the pedicle, thus
shortening the pedicle length available.
The adipofascial tum-over flap is raised on the volar aspect of the arm by means of an
H-shaped incision and includes the brachial fascia and some subcutaneous fat.
Vascularization occurs through perforators of the rete cubiti and the distal fascia of the
biceps muscle. Its maximum length of 20 cm allows it to reach the proximal forearm
anteriorly and the olecranon posteriorly.
Thanks to its pattern of vascularization, this flap can be elevated even when the
forearm and hand are perfused through a compensatory circulation.
By grading the thickness of the subcutaneous layer, defects of different depth can be
appropriately filled. The fat paddings also represent a suitable bed for nerve
reconstruction, even if grafts are required.
A further advantage is the good appearance of the donor site, with maintenance of the arm
contour.
RESUME. Les
lésions graves du coude qui intéressent les nerfs sont trčs communs, et diverses
techniques ont été proposées pour la couverture de cette région anatomique: les
lambeaux pédiculés ŕ distance, les lambeaux musculaires et musculocutanés, les
lambeaux fasciocutanés et les lambeaux libres. Les indications pour toutes ces techniques
sont encore controversées. Récemment certains Auteurs ont décrit les lambeaux
adipofasciaux retournés (tum-over), qui peuvent ętre levés sans sacrifier le derme
surjacent et façonnés dans l'épaisseur pour remplir des défauts de différent degré.
Il faut délinéer le lambeau sur l'aspect fléchisseur du bras et exposer la couche
sous-cutanée ŕ travers une incision ŕ forme de H. Ensuite il faut passer ŕ la
dissection de la peau au niveau dermal, et le niveau sous-cutané, avec le faisceau
profond, est élevé dans la mesure désirée. Il faut laisser un pédicule intact de 2 cm
proximalement au défaut et retourner le lambeau, afin de le remplir. Les Auteurs
présentent deux cas traités avec cette technique.
BIBLIOGRAPHY
- Mathes S.J., Nahai F.: "Clinical atlas of muscle and
musculocutaneous flaps". C.V. Mosby, St Louis, 1979.
- Buehler U., Frey H.P.: Retrograde posterior interosseous
flap. J. Hand Surg. (Am.), 16: 283, 1991.
- Orgill D.P., Pribaz U., Morris D.J.: Local fasciocutaneous
flaps for olecranon coverage. Ann. Plast. Surg., 32: 27-3 1.
- Graf P., Steinau H.U., Ingianni G., Biemer E.: The pros and
cons of distant pedicled flaps for upper extremity trauma reconstruction in the era of
microvascular surgery. Eur. J. Plast. Surg., 14: 288, 1991.
- Gunemer R., Montandon D., Marty F.M., Zbrodowski A.: The
subcutaneous tissue flap and misconception on the fasciocutaneous flap. Scand. J. Plast.
Surg., 20: 61, 1986.
- Marty F.M., Montandon D., Gunemer R., Zbrodowski A.: The
use of subcutaneous tissue flaps in the repair of soft tissue defects of the forearm and
hand: An experimental and clinical study of a new technique. Br. J. Plast. Surg., 37:
95, 1984.
- Lai C-S., Lin S-D., Chou C-K., Tsai C-W.: Clinical
application of adipofascial tum-over flaps for burn wounds. Burns, 19: 73, 1993.
Lai C-S., Lin S-D., Yang C-C., Chou
C-K.: The adipolascial turnover flap for complicated skin defects of the hand and finger.
Br. J. Plast. Surg., 44: 165, 199t.
This paper was received on 20 March 1999.
Address correspondence to:
Dr M. Calcagni
Policlinico Multimedica
Via -Milanese 300
20099 Sesto San Giovanni (MI), Italy
Tel. 0039 02 24209262 |
|