Annals of
Burns and Fire Disasters - vol. XII - n° 3 - September 1999
FREE ARTERIALIZED VENOUS FLAP
Ayad H. M.
Department of Plastic and Reconstructive Surgery,
Tanta Faculty of Medicine, Tanta, Egypt
SUMMARY. Free flap transplantation is
an important method for the surgical resurfacing of soft tissue defects in all parts of
the body. The arterialized venous flap technique depends on the use of two veins in the
skin flap that are used respectively for arterial flow and venous drainage. The blood in
the arterialized venous flap disperses faster and over a larger area than in flow-through
venous island flaps. Survival depends on the size of the flap, arterial inflow, and venous
outflow. For good results, an arterialized venous flap should be designed to contain most
of the venous network in the centre, the arterial inflow should be anastomosed to one
afferent vein, and two or more efferent veins should drain the arterialized venous flap.
Nine cases of skin defects were treated with a free arterialized venous flap. The
aetiology of the defects was secondary to release of scar contracture. Five patients were
suffering from post-burn contracting scars. Two cases were secondary to post-traumatic
scar and two cases presented a recent traumatic skin defect. The results showed that the
arterialized venous flap was useful as a free flap in small soft tissue defects. It is an
easily elevated, thin flap that can be harvested with little morbidity from a wide variety
of donor sites.
Introduction
Free flap transplantation is an important
method for the surgical resurfacing of soft tissue defects in all parts of the body.
Although there are many possible methods for the clinical repair of such defects, at a
given moment free flap transplantation may be the only available option. Free flaps
usually utilize both arterial and venous anastomosis, which sometimes presents the
following limitations:
- the number of available sites containing a
defined artery for free flap is sometimes limited
- many free flaps require the sacrifice of a
main artery
The arterialized
venous flap technique involves the use of two veins in the skin flap, one for arterial
flow and one for venous drainage.
Historically, an early technique for the rescue of an ischaemic extremity consisted of the
creation of an arteriovenous fistula between the venous and arterial systems of the
extremity, following which the venous system served as a route of arterial inflow. Ozek et
al.' studied the changes occurring in the venous system after its arterialization and
showed that the thickening and hypertrophy of the vessel walls indicated adaptive changes
to withstand the increased stress experienced in their new roles as arterial conduits. In
experimental rat models, histological evidence clearly shows that arterialization of the
venous system can significantly counteract ischaemic injury to extremity muscles that have
suffered loss of arterial supply.
The first experimental study performed on the arterialized venous flap was described by
Nakayarna et al. Many experimental studies have been performed to evaluate this flap's
viability, reliability, and haemodynamics, as well as the factors affecting its survival.
Isotope perfusion and an infra-red thermographic study were performed by Wolft' et al.,'
showing that in a rat model of epigastric arterialized venous flap the blood flow was
92.7%, while in free venous flap it was 62.4% and in venous island flap 31%. An infra-red
thermographic study showed that blood in the arterialized venous flap dispersed faster and
over a larger area than in flow-through venous island flaps.
Inada et al. studied factors affecting the survival of the arterialized venous flap and
found that these flaps could become necrotic in the presence of a relative excess of
arterial blood inflow and that two venous exits were more effective than one. They
concluded that survival depended on the size of the flap, arterial inflow, and venous
outflow. They reported the case of a patient in whom a 10 by 15 em free flap harvested
from the lower extremity survived on the forearm.
Roberts et al. studied the relative importance of reduced arterial inflow versus reduced
venous outflow as a factor affecting flap necrosis. They designed a rat bipedicled venous
island flap, which they examined in four different conditions, i.e. unilateral
arteriovenous ligation, unilateral vein ligation, unilateral arterial ligation, and
alternate side vein and artery ligation. They concluded that the flap was more sensitive
to arterial inflow than to venous outflow.
Woo et al. used 16 canines to investigate the survival rate and pattern of the
arterialized venous flap and compared the results with those of the conventional saphenous
flap.
Gross examination of venous network blood gas, venograms, blood pressure tests, and
histological studies were also carried out. The blood gas analysis showed that more
effective oxygen consumption took place when the number of draining veins increased. The
high pressure arterial blood flow system induced smooth muscle proliferation and new
growth of elastic fibres in the vein. Also, progressive narrowing of the lumen accelerated
the development of collateral circulation and neovascularization as far as the flap
margin. They recommended the following procedures for complete survival:
- an arterialized venous flap should be
designed to contain most of the venous network in the centre
- the arterial inflow should be anastomosed
to one afferent vein
- two or more efferent veins should drain the
arterialized venous flap
Fukui et al. recommended
delaying the flap until after creation of an arteriovenous fistula, at proximal level, two
weeks prior to elevation of the flap. This recommendation was based on an experimental
study performed on 24 rats. In 50% of the cases the fistula passed completely, 40% showed
partial necrosis, and 10% were completely necrosed.
In the rabbit, Cho et al. studied the effect of surgical and chemical delay on the
survival of the arterialized venous flap, concluding that a delay in the surgical
procedure increased the flap survival percentage in proportion to the period of delay.
They also found that by combining surgical and chemical delay (doxazosin mesylate,
nitroglycerine patch), the period of delay could be shortened and the technique could
possibly be applied effectively in clinical cases.
Clinical trials have been performed in different centres with various results. Yilmaz et
al. used a forearm arterialized venous flap to cover a defect following a facial burn
scar. Inoue et al. used a flap with palmaris longus in an injured hand with tendon and
soft tissue defect. Sakai` used an arterialized venous groin flap to cover a cheek defect
after excision of squamous cell carcinoma. Klein` described a technique for intra-oral
defects.
On the basis of these data a clinical study was performed of the arterialized venous flap
used to cover soft tissue defects.
Patients and methods
From March 1997 to September 1998 nine
cases of skin defect were treated with free arterialized venous flap. All the patients
were adult (age range, 21 to 45 yr). The aetiology of the defect was secondary to the
release of scar contracture. Five patients presented post-burn contracting scars. Two
cases were secondary to posttraumatic scars and in two cases there was a recent traumatic
skin defect.
Operative technique
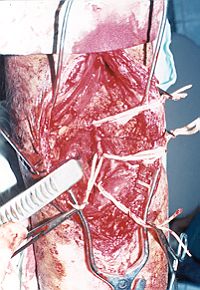
Recipient site. The site was
prepared first by excision of the scar and release of the contracture or excision of
tissue devitalized in the recent trauma. The adjacent artery was exposed, as well as two
superficial veins (Figs. 1, 2).
|
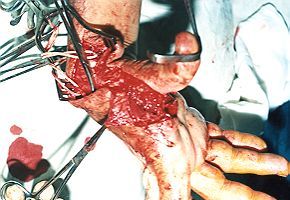 |
| Fig.
1 - Excision of scar and exposure of recipient artery and veins. |
Fig.
2 - Release of' contracture and exposure of radial artery and superficial veins. |
|
Donor
site. The donor site was chosen so that there was a cutaneous vein with two
tributaries. Commonly used sites were forearm skin, the dorsurn of the foot, and the calf
area. The size of the flap was determined and marked so that flap consisted of a skin pad,
subcutaneous fat, and a vein with one proximal and two distal ends (Fig. 3). The
vein was dissected as far away as possible in order to have a good length. The skin was
cut all around. The vein was irrigated with heparinized saline solution and prepared for
anastomosis (Fig. 4).
 |
 |
Fig. 3 - Design of skin flap. |
Fig. 4 - Prepared free skin flap. |
|
Anastomosis.
The recipient veins were irrigated with heparinized saline solution to ensure there was no
proximal obstruction, and end-to-end anastomosis was effected between the two veins of the
flap and the recipient veins by means of 7/0 proline sutures. Arteriotomy was performed at
the recipient artery, and the proximal end of the vein was sutured to it end-to-side,
using 7/0 proline sutures. The patency of the anastomosis was assessed immediately by
sensation of the thrill on the venous side and the bleeding edges of the skin flap. The
flap was sutured and the area was drained by TI-S suction pulp drainage (Fig. 5).
The donor site was usually closed primarily or by split-thickness skin graft. A light
dressing was applied to allow close observation of the flap for colour and venous
congestion. There was no need for post-operative systemic heparin.
 |
Fig.
5 - Anastornosis of flap to recipient site. |
|
Results
In the early
post-operative period there was congestion of the flap but the circulation remained good,
as determined by Doppler, showing good arterial inflow and venous outflow. Congestion
reached a maximum at 48 h, after which the flap regained its shape and colour. Some cases
showed bulla formation and epidermolysis (Fig. 6).
 |
Fig. 6 -
Superficial epidermolysis of flap. |
|
Of the nine
cases, one showed superficial necrosis of the whole flap, under which a haernatoma formed.
The donor site was the medial aspect of the thigh with the saphenous vein. Two cases
presented peripheral necrosis in about 20% of the flap but there was no need for repeat
surgery. Six cases had no more than 5% partial necrosis (Figs. 7, 8).

|
 |
| Fig.
7 - Partial necrosis of Hap. |
Fig. 8 - Partial necrosis of flap. |
|
The size of
the flaps ranged from 2 x 4 cm to 4 x 5 cm, with a mean of 15 sq. cm. Smaller flaps were
more successful.
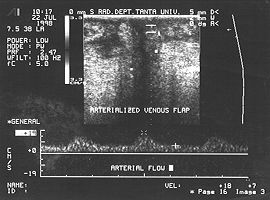
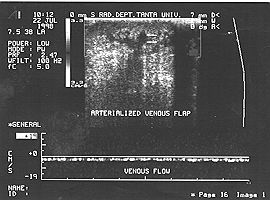
A duplex scan was performed in each flap on the fourth day. The scan showed that there was
good arterial flow and capillary filling, as well as smooth venous return in eight cases.
The arterial and the venous phases were recorded. The difference ranged between 18 (peak
systolic velocity) and 7 (end diastolic velocity), indicating good capillary filling and
low resistance, i.e. good arterialization of the skin flap (Fig. 9).
|
|
| Fig.
9 - Arterial phase of duplex scan with good arterial pulsation, and venous phase
showing continuous flow. |
|
Discussion
Many types of local flap
can be used to cover a soft tissue defect, but in some cases free flap is the most
suitable. Yoshimura et al. described an arterialized venous skin flap for the treatment of
skin defects in the fingers. This flap employed forearm skin with subcutaneous vein. The
skin area ranged from 1.3 x 2 em to 2 x 5 cm. The results were good. The elastic skin flap
presented the following advantages: thin subcutaneous fat, possible use in any recipient,
no immobilization, one-stage procedure, possibility of using the injured digital artery in
anastomosis.
Commenting on this procedure, Nichter` stated that in the light of previous anatomical
studies the use of a properly placed efferent and afferent arteriovenous fistula enabled a
single system to provide both physiological functions.
This is not surprising since both the arterial and venous trees are actively involved in
the exchange of oxygen and carbon dioxide. According to Nichter, these flaps might
possibly be used successfully as composite skin flaps, but no investigations were
performed to determine the patency of the anastomosis.
In the present study, a coloured duplex scan was used to follow up the flap, which showed
good arterial perfusion and patent venous flow.
In support of this technique, lwasawa` used an arterialized venous flap from the thenar
and hypothenar region to cover finger pulp. Thirteen out of fifteen flaps were 100%
successful, and it was concluded that the arterialized venous flap was a useful
alternative for the repair of finger pulp tissue loss.
Klein et al. used a forearm arterialized venous flap to cover intra-oral defect after
excision of squamous cell carcinoma with 52% complete success, 21% partial loss, and 27%
total loss. The size of the flap ranged from 3 x 4 cm to 5 x 7 cm (average size, 20 sq.
cm). They concluded that this flap could be a possible alternative for the coverage of
skin defects.
The higher number of failures could be attributed to the use of one venous exit, which
increased venous congestion, as also to the larger size of some flaps. Inada et al.5
stressed the benefits of increased venous drainage to the arterial inflow.
These results are not consistent with those of Yiknaz et al., who used an arterialized
venous forearm flap to cover defects of up to 10 x 12 em in five cases, with only 30%
partial necrosis in one flap, concluding that this type of flap provided large, thin,
good-quality tissue with less morbidity in the donor site than the conventional radial
forearm flap. In the present study the results were more or less comparable with those of
Klein et al., with a 60-100% success rate and 20% failure rate, the rest presenting
partial necrosis. Cho et al. recommended delaying the flap in order to use larger flaps,
obtaining a 100% survival rate in ten flaps out of thirteen (size range, 6 x 8 em to 14 x
16 em) to cover defects after scar excision and acute injury. Fulci et al.' found that
delaying the flap two weeks improved results with the arterialized venous flap.
In conclusion it can be said that the arterialized venous flap is useful as a free flap in
small soft-tissue defects. It is an easily elevated, thin flap that can be harvested from
wide donor sites, with only minor morbidity.
RESUME. La
transplantation du lambeau cutané libre est une méthode importante pour la couverture
chirurgicale du tissu mou dans toutes les zones du corps. La technique du lambeau
artérialisé dépend de l'emploi de deux veines dans le lambeau cutané respectivement
pour la circulation artérielle et le drainage veineux. Le sang dans le lambeau
artérialisé se propage plus rapidement et dans une aire plus grande que les lambeaux en
îlot veineux perméables. La survie dépend de la dimension du lambeau, l'afférence
artérielle et l'efférence veineuse. Pour obtenir de bons résultats il faut préparer un
lambeau veineux artérialisé qui contient la plupart du réseau veineux au centre et
anastomoser l'abduction artérielle ŕ une veine afférente; en outre, au moins deux
veines efférentes doivent drainer le lambeau veineux artérialisé. Les Auteurs
déscrivent neuf cas de défauts cutanés traités avec la technique du lambeau veineux
artérialisé libre. L'étiologie des défauts était secondaire ŕ la libération de la
contracture cicatricielle. Cinq patients étaient atteints de cicatrices en contracture
dues aux brűlures. Deux cas étaient secondaires ŕ une cicatrice post-traumatique et
deux cas présentaient un défaut cutané traumatique récent. Les résultats ont montré
que le lambeau veineux artérialisé est utile comme lambeau libre dans les petits
défauts de tissu mou. C'est un lambeau mince, facilement élévé, que l'on peut cueillir
avec une morbidité limitée.
BIBLIOGRAPHY
Pittet B., Chang R, Cedema P., Cohen M.B., Blair
W.F., Cram A.E.: The role of neovascularization in survival of an arterialized venous
flap. Plast. Reconstr. Surg., 97: 621-9, 1996.
Ozec C., Zbang R, Lineaweaver
W.C., Chin B.T., Newlin L., Eiman T., Buncke H.J.: Arterialization of the venous system in
a rat lower limb model. Br. J. Plast. Surg., 50: 402-7, 1997.
NakayamaY., Soeda S., Kasai Y.:
Flaps nourished by arterial inflow through the venous system: An experimental
investigation. Plast. Reconstr. Surg., 67: 328, 1981.
Wolff K.D., Telzrow T.,
Rudolph K.H., Franke J., Wartenberg E.: Isotope perfusion and infrared thermography of
arterialized venous flow-through and pedicled venous flap. Br. J. Plast. Surg., 48: 6170,
1995.
Inada Y., Fukui A., Tami S.,
Mizumoto S.: The arterialized venous flap: Experimental studies and a clinical case. Br.
J. Plast. Surg., 46: 61-7, 1993.
Roberts A.P., Cohen LL, Cook T.A.:
The rat ventral island flap: A comparison of the effects of reduction in arterial inflow
and venous outflow. Plast. Reconstr. Surg., 97: 610-5, 1996.
Woo S.H., Kim S.E., Lee T.11,
Jeong LK, Scul J.H.: Effects of blood flow and venous network on survival of the
arterialized venous flap. Plast. Reconstr. Surg., 101: 1280-9, 1998.
Fulsi A., Inada Y., Murata K.,
Ueda Y., Tamai S.: A method for prevention of arterialized venous flap necrosis. J.
Reconstr. Microsurg., 14: 67-74, 1998.
Cho B.C., Lee M.S., Lee LK, Byun
J5, Baik B.S.: The effects of surgical and chemical delay procedures on the survival of
arterialized venous flaps in rabbits. Plast. Reconstr. Surg., 102: 1134-43, 1998.
Yilmaz M., Menderes A., Karatas
0., Karaca C., Bartneu A.: Free arterialized venous forearm flaps for limb reconstruction.
Br. J. Plast. Surg., 49: 396-400, 1996.
Inoue G., Tamura Y., Suzuki K.:
One-stage repair of skin and tendon digital defects using the arterialized venous flap
with palmaris longus tendon: An additional four cases. J. Reconstr. Microsurg., 12: 93-7,
1996.
Sakai S.: Arterialized venous groin flap: Case
report. Br. J. Plast. Surg., 49: 90-2, 1996.
Klein C., Kovacs A., Stuckensen
T.: Free arterialized venous forearm flaps for intra-oral reconstruction. Br. J. Plast.
Surg., 50: 166-71, 1997.
Yoshimura M., Shimada T., Imura
S., Shimamura K., Yamauchl S.: The venous skin graft method for repairing skin defects of
the fingers. Plast. Reconstr. Surg., 79: 243-8, 1987.
Nichter L.S.: The venous skin graft method for
repairing skin defects of the fingers. Plast. Reconstr. Surg., 79: 249-50, 1987.
lwasawa M., Ohtsuka Y., Kushima
H., Kiyono M.: Arterialized venous flaps from the thenar and hypothenar regions for
repairing finger pulp tissue losses. Plast. Reconstr. Surg., 99: 1765-70, 1997.
Cho B.C., Lee J.11., Byun LS., Baik B.S.: Clinical
applications of delayed arterialized venous flap. Arm. Plast. Surg., 39: 145-57, 1997.
This paper was
received on I March 1999.
Address correspondence to:
Dr Ayad H.M.
Department of Plastic and Reconstructive Surgery
Tanta Faculty of Medicine
Tanta, Egypt. |
|