Annals of Burns and Fire Disasters - vol. XII - n° 3 - September 1999 SUPERIORLY BASED NIPPLE-AREOLA COMPLEX FLAP:A MILESTONE FOR RECONSTRUCTION OF THE POST-BURN DEFORMED BREAST Elsayed M. Abdel-Razek Tanta Faculty of Medicine, Tanta, Egypt SUMMARY. Post-burn deformities of the female breast pose a problem for plastic and reconstructive surgeons as well as psychological problem, for the patient. The female breast is roughly circular, except at the upper outer quadrant where the axillary tail of Spence extends to the axilla. To achieve good cosmetic results we should endeavour to regain the shape of the breast and the nipple-arcola complex. In this study we reconstructed 35 breasts in 23 females suffering from post-burn deformed breasts, including malpositioned or destroyed nipple-arcola complex, in patients aged 16 to 23 yr. In all patients we made a superiorly based nipple-areola complex Hap with two kiteral flaps advanced below it to provide protrusion, in addition to shifting whole breast tissues upwards into the correct position. The post-operative results and follow-Lip have proved satisfactory to both surgeon and patients. We recommend employing this technique in the reconstruction of the burned female breast. Introduction Reconstruction of the burned breast has
two aspects: first, reshaping of the breast as a whole and, second, reconstruction of the
nipple-areola complex. Reconstruction of these structures following deep burns is still a
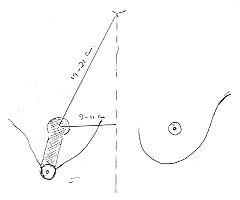
challenge for plastic surgeons. Aim of the work The aim of this study was to evaluate the superiorly based nipple-areola complex flap as a new technique for the reconstruction of the post-burn deformed female breast. Patients and methods Between 1996 and 1999, 23 female patients aged 6 to 23 yr underwent reconstruction of 35 post-burn deformed breasts with superiorly based nipple-areola complex flaps. The displaced or deformed nipple was marked and the new nipple site was determined and marked 9-11 cm from the mid-stemal line and 19-21 cm from the suprastemal notch. A periareolar marking was located 2 cm above and around the future nipple site, and two lines were drawn joining the border of the old areola to that of the proposed new areola (Fig. 1).
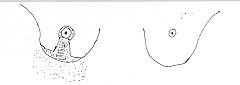
Under general anaesthesia, sterilization, and draping, the lateral margin markings were incised and deepithelialization of the skin was performed between the two incisions and the circle of the new nipple-areola complex. The two lateral incisions were deepened to the level of the pectoral fascia and the whole nipple-areola complex flap was dissected freely from the pectoral fascia, maintaining its superior pedicle. The areola was then sutured into its new position (Fig. 2).
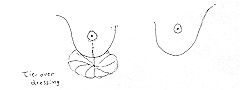
The two lateral pillars of the breast were then advanced medially after release incisions and sutured together. After lifting the whole breast upwards, the raw area left underneath was covered with split-thickness skin graft (Fig. 3).
A tie-over dressing was used for the grafted area and the breast was dressed by supporting it upwards and maintaining its protrusion. The dressing was removed one week later and the patient continued to wear a strong elastic brassiere for three months in order to maintain breast protrusion and minimize the effect of graft contracture. The follow-up period ranged between 4 and 16 months. Results We operated on 35 breasts in 23 patients,
always using the same technique (the superiorly based nipple-areola complex flap). Twenty
patients (31 breasts) were burned before puberty, and three patients (four breasts) were
burned after puberty. All the breasts were flat and adherent to underlying tissues, with
obliteration of the inframammary fold due to scarring. Thirty nipple-areola complexes were
displaced far from the normal anatomical position. The other five were destroyed, and here
we used a hyperpigmented, healed burn area for the areola and transferred it by the same
technique to the new normal anatomical position. The nipples were reconstructed
subsequently.
Discussion The surgical
reconstruction of post-burn breast deformity is still a challenge for plastic surgeons.
The procedures for total reconstruction are surprisingly scarce in the literature. Conclusion In conclusion, the superiorly based nipple-areola complex flap is an excellent option in the reconstruction of post-burn female breast deformity and adds to the armamentarium of the plastic surgeon in the treatment of such cases.
RESUME. Les malformations dues aux brűlures de la mamelle féminine présentent des problčmes pour le chirurgien plastique et reconstructif et des problčmes psychologiques pour la patiente. La mamelle féminine est arrondie, sauf dans le quadrant supérieur extérieur, oů la queue axillaire de Spence s'étend jusqu'ŕ l'aisselle. Pour obtenir de bons résultats esthétiques il faut faire attention pour recouvrer la forme de la mamelle et du complexe mamelon/aréole. Dans cette étude l'Auteur a reconstruit 35 mamelles dans 23 femmes atteintes de malformations de la mamelle causées par les brűlures qu'elles avaient souffertes, y inclus le mauvais positionnement ou la destruction du complexe mamelon/aréole. Lâge des patientes variait entre 16 et 23 ans. Dans toutes les patientes il a effectué un lambeau basé supérieurement dans le complex mamelon/aréole avec deux lambeaux latéraux avancés inférieurement pour lui donner une certaine rondeur comme aussi des tissus entiers mobiles de la mamelle positionnés correctement en direction ascendante. Les résultats post-opératoires et ŕ long terme étaient satisfaisants pour le chirurgien et les patientes. L'Auteur recommande cette technique pour la reconstruction de la mamelle féminine brűlée. BIBLIOGRAPHY
|