Annals of Burns and Fire Disasters - vol. XIII - n° 1 - March 2000 LIMB SALVAGE IN A BURN PATIENT WITH A MUSCLE-FREE FLAP Cavadas P.C. La Fe University Hospital, Valencia, Spain SUMMARY. A clinical case is described of massive thigh burn with exposure of the femur in which the possible necessity of hip disarticulation was avoided. This drastic surgical treatment often proves necessary in very deep thermal burns of the lower limb that leave bones and joints exposed. In the case described, a rectus abdominis muscle free flap was applied after partial bone debridement of the femur. The case was complicated by the occurrence of an open pathological subtrochanteric, fracture. A solid intramedullary rod was successfully applied and the fracture consolidated. The patient recovered his ability to walk. Introduction Very deep thermal burns of
the lower limb can leave exposed bones and joints. This situation is far more common in
the lower leg than in the thigh, and extensive femoral diaphysis exposure is seldom found.
Pathological conditions predisposing to prolonged loss of consciousness, e.g. seizures,
alcoholism, stroke, loss of sensibility, and extreme slimness, all increase the risk of
very deep bums of the thigh, with muscle loss sufficient to expose long segments of
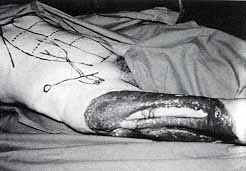
femoral diaphysis. Case report A fifty-yr-old male presenting mild alcoholism but no other previous diseases was admitted suffering from a very deep burn of the thigh (7% TBSA). Prophylactic penicillin was instituted in view of the extensive muscle destruction. Several debridements of soft tissues led to exposure of a 25-cm-long segment of femoral diaphysis (Fig. 1).
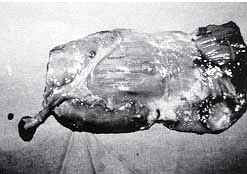
Tensor fasciae latae was lost, as also quadriceps and part of biceps femoris. The patient had been considered in another hospital for a hip di s articulation, which he had rejected. The reconstruction options were limited to a muscle free flap, as the majority of regional flaps were not available. A rectus abdominis muscle free flap was applied, after partial bone debridement of the femur (Figs. 2, 3).
On post-operative day 10, an open pathological subtrochanteric fracture occurred, with purulent discharge in the fracture focus. The limb was still considered salvageable, and fracture fixation was therefore performed with a solid intramedullary rod. The patient was put on aggressive antibiotic therapy and wound irrigation. The fracture finally consolidated, and the remaining chronic osteomyelitis progressively reduced its discharge, leaving a sinus with low production. The patient is now walking without assistance (Fig. 4), although he has not returned to his former active life.
Discussion Free flap reconstruction
for lower limb salvage has been widely reported both in acute trauma and in chronic
conditions such as extensive ulcers or osteomyelitis. The superiority of preservation of
the leg to amputation and prosthesis - although not always clear in below-the-knee wounds
- is absolutely indicated in high above-the-knee conditions. In the case reported the
alternative would have been a hip disarticulation, an extremely mutilating procedure.
RESUME. L'Auteur décrit un cas clinique d'une brűlure massive de la cuisse avec l'exposition du fémur. Dans ce cas il a été possible d'éviter le risque d'une désarticulation de la hanche, une procédure trčs sévčre qui est souvent nécessaire ŕ la suite des brűlures thermales trčs profondes du membre inférieur avec l'exposition des os et des articulations. L'Auteur, dans ce cas, a appliqué un lambeau rectus abdominis sans muscle aprčs le débridement partiel osseux du fémur. Le cas a été compliqué par une fracture subtrochantérique pathologique ouverte. Une broche solide intramédullaire a été appliquée avec succčs et la fracture s'est consolidée. Le patient a repris la déambulation normale. BIBLIOGRAPHY
Mathes S.J., Alpert B.S., Chang N.: Use of the muscle flap in chronic osteomyelitis: Experimental and clinical correlation. Plast. Reconstr. Surg., 69: 815, 1982.
|