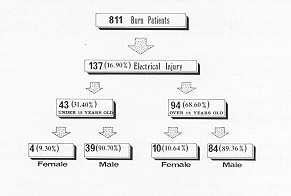
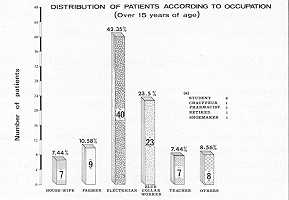
Annals of the MBC - vol. 2 - n' 1 - March 1989 EPIDEMIOLOGY OF ELECTRICAL BURNS IN OUR CENTREHaberal M., Kaynaroglu V., Oner 1, G0lay K, Bayraktar U., Bilgin N. Hacettepe University Hospital Burn Center-Turkish Transplantation and Burn Foundation Hospital, Ankara, Turkey. SUMMARY. Of the 811 patients who were admitted to our Bum Centre from January 1, 1980 to January 1, 1988, 137 (16.90%) had electrical bums, not including 7 flash bums, 2 lightning and 1 bum from electrical stove. Of these 137 patients, 94 (68.60%) were over 15 years old with mean age 26.8 years (16 to 48 years). 84 (89.36%) were males and 10 (10.64%) were females. 43 (31.40%) patients were under 15 years old with mean age 11.2 (1 to 15), 39 (90.70%) were males and 4 (9.30%) were females, the majority being 11 to 15 years old. 53 (38.69%) of the patients were injured with house current (220-400 volts) and 84 (61.31%) with high tension (100-134,000 volts). The occupations of the patients over 15 years old could be classified as follows: 40 (42.35%) electricians, 23 (23.5%) blue collar workers, 9 (10.58%) farmers, 7 (7.44%) housewives, 7 (7.44%) teachers and 8 (8.56%) others including 2 students, 2 chafreurs, 1 pharmacist, 1 pensioner, 1 engineer and 1 shoemaker. All of these patients came from throughout the country. Following routine resuscitation and local wound care, including fasciotomy and debridement, the patients were observed closely. The evidence we have obtained from this experience reveals that electricity is one of the major causes of bums; another derivation is that electrical burns are mostly encountered among electricians. This is mostly owing to the lack of knowledge and education among this group of people. We can therefore say that enhancing the level of education is a necessity with potential value. Introduction Electricity is one of the necessary requirements for human survival. However, when misused, it can lead to a life spent as a cripple or cause a fatal injury. In the developing countries, electrical energy is used widely but sometimes inappropriately. For this reason, the incidence of electrical injury causing severe complications or death is high. In order to prevent this life-threatening event, measures should be taken by health-care officials and physicians to educate the public on bum prevention through every available means of communication (1,2). In this paper, we present our 8 years' experience with electrical burns in Turkey. Materials and Methods From January 1, 1980 to January 1, 1988, 811 patients were admitted to our Burn Centre. Of these, 137 (16.90%) had electrical burns, not including seven flash burns, two lightning and one burn injury from an electrical stove. Ninety-four (68.60%) of the 137 patients were over 15 years old, with the age 26.8 years (16 to 48 years). Eighty-four (89.36%) were males and 10 (10.64%) were females. Forty-three (31.40%) patients were under 15 years old with the mean age 11.2 (1 to 15); 39 (90.69%) were males and four (9.30%) females, the majority being 11 to 15 years old (Fig. 1). Fifty-three (38.69%) of the patients were injured with house current (220-400 volts) and 84 (61.31%) with high tension (100-134.000 volts). The occupations of the patients over 15 years were as follows: 40 (42.35%) electricians, 23 (23.5%) blue collar workers, 9 (10.58%) farmers, 7 (7.44%) housewives, 7 (7.44%) teachers and 8 (8.56%) others, including 2 students, 2 chauffeurs, 1 pharmacist, 1 pensioner, 1 engineer and 1 shoemaker (Fig. 2).
All of our patients came to our Centre from throughout the country. The treatment of all patients began at the time of hospitalization. Following routine examinations, 1.v. fluid (saline or saline with dextrose) was administered and following the results of the electrolyte measurements, provided potassium levels were normal, the solution was changed to Ringer's lactate. The rate of fluid administration was adjusted until the urine volume was at least 50 ml. per hour. If the patient was oliguric and acidotic, sodium bicarbonate, 20-40 gm of mannitol and 40-100 ing furosemide were given. If the patient still remained oliguric, and potassium, BUN, and creatinine levels were rising, peritoneal or haemodialysis was carried out using a double-lumen subclavian catheter (Gambro SCK-102 20-cm, Lund, Sweden). We found that this system was very easy to use for both haemodialysis and parenteral alimentation. A urinary catheter and a central venous pressure catheter were used only in severe cases or if clinical evaluation so indicated.
Following initial stabilization, the patients were taken to the dressing room for re-evaluation and, if necessary, debridement, escharotomy and fasciotomy. After premedication, wounds were cleansed and closed using one of the local chemotherapeutic agents, such as silver sulphadiazine, mafedine acetate, or silver-incorporated amniotic membrane (4). This procedure was repeated until all nonviable tissue was removed. In patients where amputation was required the wounds were then closed with skin grafts or flaps. Rehabilitation such as physical therapy was started while patients were hospitalized and continued after discharge if necessary. Results A total of 152 surgical procedures
were employed on 76 patients: 21 patients, one; 29 patients, two; 14 patients, three; four
patients, four; and five patients five procedures. Forty-six (60.53%) had inuscoloskeletal
complications; 32 (42. 11 %) patients required major amputations which included seven
right arm disarticulations, four right arm amputations, five right forearm amputations,
five right leg amputations (below the knee); six left arm amputations, two left forearm
and three left leg amputations (below the knee); eight patients required multiple
amputations; minor amputations consisted o17 various finger or toe amputations. In
addition, there were one right mandible fracture, two compression fractures of lumbar
vertebrae, three head traumas with craniectomies, and two costal fractures. Discussion Electrical burn injury is one of the
severe problems in our society in Turkey. The main causes of injury in patients over 15
years of age are misuse, lack of attention and lack of knowledge, and the fact that
utility poles and wiring are placed low and extremely close to buildings, so even
installing a TV aerial can be life-threatening. In patients under 15 years of age, the
injuries were mainly the result of mischievous activity that involved climbing, and lack
of parental supervision. Another contributing factor is the lack of control of the systems
by the electric companies. RESUME. Entre le premier
janvier 1980 et le premier janvier 1988, 811 patients ont été hospitalisés dans le
Centre des Brûlés de l'Hôpital Universitaire Hacettepe, dont 137 (16,90%) avec
brûlures électriques, sans tenir compte de 7 brûlures par lueur, 2 par foudre et 1 par
radiateur électrique. De ces 137 patients, 94 (68,60%) avaient plus de 15 ans, avec un
âge moyen de 26,8 ans (de 16 à 48 ans); 84 (89,36%) étaient masculins et 10 (10,64%)
féminins. 43 (31,40%) patients avaient moins de 15 ans, avec un âge moyen de 11,2 ans
(d'un à 15 ans); 39 (90,70%) étaient masculins, et 4 (9,30%) féminins; la plupart
avaient entre 11 et 15 ans. 53 (38,69%) des patients ont été blessés avec le courant
domestique (220-400 v) et 84 (61,3 1 %) avec haute tension (100- 134.000 v). Les patients
âgés de plus de 15 ans exerçaient les métiers suivants: 40 (42,35%) électriciens; 23
(23,50%) ouvriers, 9 (10,58%) agriculteurs, 7 (7,44%) ménagères, 7 (7,44%) professeurs
et 8 (8,56%) métiers divers: 2 étudiants, 2 chauffeurs, 1 pharmacien, 1 retraité, 1
ingénieur et 1 cordonnier. Les patients provenaient de toutes les régions du pays. On a
pratiqué la réanimation de routine et les soins locaux des brûlures, ce qui inclut la
faisceautornie et la détersion, et les patients ont été suivis avec attention. BIBLIOGRAPHY
|