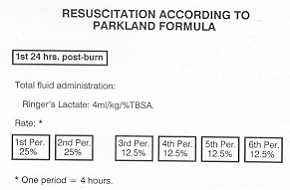
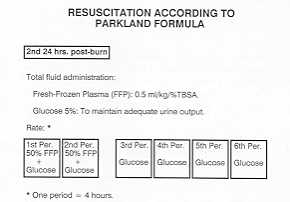
Annals of the MBC - vol. 2 - n' 1 - March 1989 PARKLAND FORMULA AS A GUIDE FOR RESUSCITATIONloannovich 1, Alexakis D., Parker 1, Mantas N. Centre of Plastic and Reconstructive SurgerV and MicrosurgerV, Athens General Hospital, Greece SUMMARY. During a two-year period (1987-1988) 180 patients with bum injury were admitted to our clinic for acute care, 64 of them (35.5%) considered to be major injuries (over 25% T13SA), requiring fluid resuscitation. In this series all admissions were included, regardless of age, concomitant injuries or pre-existing diseases. Initial resuscitation was accomplished using the Parkland formula as a guide for resuscitation. This formula employs Ringer's lactate alone for the first 24 hour period giving a total amount of 4 ml/kg/% burn area. For the second 24 hour period it employs plasma at the amount of 0.5 ml/kg/% bum area and 5% glucose in an amount enough to maintain adequate. urine output. After the initial resuscitation, fluids were limited to the maintenance solutions. The efficacy of initial therapy was estimated by the determination of.. a) the accuracy of the resuscitation guides; b) the response of various organ systems (cardiovascular system, urinary system, pulmonary system, the balance of fluids and electrolytes; c) early mortality; and d) the complications encountered during the entire first, week post-burn period. According to our results the Parkland resuscitation formula provides a satisfactory urinary output, diminishes the development and accelerates the regression of the oedema. Thus it minimizes the possibility of renal failure and brain oedema. It contributes also to good electrolyte balance and is less expensive than the other formulae. On the other hand it necessitates large amount of fluids, which need a well organized team work with the nursing staff and a close monitoring of the clinical and laboratory paremeters for the control of the massive fluid infusion. It is a well accepted axiom in the treatment of burns that the efficacy of resuscitation diminishes the frequency and severity of complications, resulting in a reduction of mortality. The improvement of the understanding of burn pathophysiology has led to the development of various formulae for the initial treatment of hypovolaernia. Moyer et at. (1965) proved the contribution of the Na+ ion in the intra- and extracellular distribution of electrolytes and water during the initial period of burn disease. As a consequence Baxter (1974) introduced the Parkland formula for fluid volume replacement. This formula has become popular and many investigators are still lauding its advantages (Pruit 1978, Goodwin et al. 1983, Bowser-Wallace and Caldwell 1986). Material and Methods During the two-year period, 1987-1988, 180 adult patients with burn injuries were admitted to our department for acute care. 64 of them (35.5%) were over 25% TI1SA, requiring fluid resuscitation. In this series all admissions were included, regardless of age, concomitant injuries or pre-existing diseases. Initial resuscitation was accomplished using the Parkland formula as a guide. The first 48 post-burn hours are divided into six 4-hour periods in order to facilitate the nursing routine and eliminate possible complications arising from the large volumes of fluid infused. According to the formula we administer Ringer's lactate alone for the first 24 hours post-burn, giving a total amount of 4 ml/kg/% TI1SA (Fig. 1). For the second 24-hour post-burn we begin administering plasma in an amount of 0.5 ml/kg/% TBSA, during the first two periods in order to "expand" the intravascular volume (Fig. 2). Adequate urine output (50-100 ml/h) is maintained with the administration of 5%-glucose, according to the formula of SDSP (Scott, McDougall, Slade and Pruit 1978). The rate of fluid administration is in accordance with Baxter's proposal (1979) in order to maintain the functional extracellular fluid volume within + 10% of the individually calculated volume. 50% of the calculated volume of Ringer's lactate is given during the first two periods and the rest is evenly administered over the remaining 4 periods. Monitoring during the first post-burn days is focused to determine the possible complications and the efficacy of the initial therapy (Fig. 6). Many such parameters have been proposed, some of which, in our view, are not totally justified, since they give academic and scientific information, without substantial benefit to the patient's care. For this reason we estimate routinely the efficacy and the side effects of the initial therapy by the determination of:
Haematocrit, every 6 hours, as a parameter of efficacy of the reduction of haemoconcentration c) Vital signs every hour (pulse rate, blood pressure, surface temperature and respiration rate).
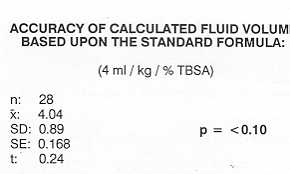
Results A. Accuracy of the calculated fluid volume The overall fluid requirement was within 4 ml/kg/% T13SA, since the difference between the calculated and the given fluid volumes was not statistically significant (Fig. 3). Taking into consideration the mean value (4.04 nil) and the standard deviation (0.89 ml), we observed a considerable discrepancy between the given and the calculated fluid volumes in 4 cases. An 18-year-old patient with electrical burns of an extent of 35% T13SA required 4,700 nil Ringer's lactate more than the calculated volume (5.9 ml/kg/% T13SA). A p = <0.10 20-year-old woman with thermal burns of 35% T13SA, treated on an air-fluidized bed, required 2,500 nil Ringer's lactate more (5.42 ml/kg/% T13SA). A comatose 83-year-old woman with 22% T13SA, burned as a result of a fall following a cerebrovascular accident, required 2,000 nil more (5.80 ml/kg/% T13SA). The fourth case was a 28-year-old man with 30% T13SA who attempted suicide during a severe depression of manic depressive psychosis; he required 2,600 nil more (5.23 ml/kg/% T13SA).
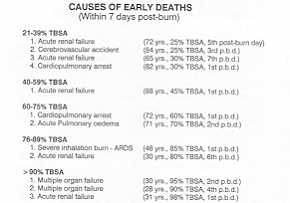
B. Early mortality The lethal potential of inadequate resuscitation was considered to last for only 7 days. During this period 12 patients, with varying extent of T13SA, died (Fig. 4). However it should be stressed that the average age of deaths in the group up to 75% T13SA was 78.4 years, while the overall average age of the patients in these groups was 43.4 years. It is of course ' evident that the mortality rate in the group with over 76% T13SA was extremely high (66.6%). As regards the cause of death (Fig. 5), 5 died from acute renal failure, between the Ist and 7th post-burn day, despite attempts at haemodialysis in two cases. Two patients died from cardio-pulmonary arrest in the first 12 hours, probably due to cerebral oedema. One of these cases had exudative pericarditis, which was confirmed on post mortem. One patient, a 71-year-old nephrectomized woman with pulmonary oedema, died on the second post-bum day as a result of excessive fluid administration. This is the only case where our parameters remained within normal limits but failed to indicate the onset of such a complication. Two cases with burns of over 90% T13SA died from multiple organ failure during the first post-burn day. C. Parameters evaluating the efficacy offluid administration (Fig. 6) The urine output during the first 24 hours was adequate, ranging between 40 and 55 ml/h, while on the second day a steady increase in output was noted after the administration of the calculated plasma volume.
The specific gravity of the urine showed
some fluctuation, but resulted in a fairly steady decrease from 1020 to 10 15.
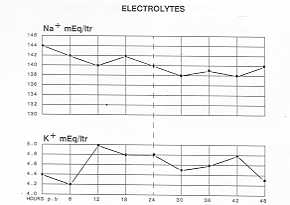
The haematocrit seemed to fall on the second post-burn day, while during the first day it remained at relatively high levels. D. Electrolytes (Fig. 7) Despite the large load of sodium
during the first day, the levels remained constant and within normal limits. It is of
interest that on the second post-burn day the levels also remained constant although the
administered sodium rate by plasma is much reduced.
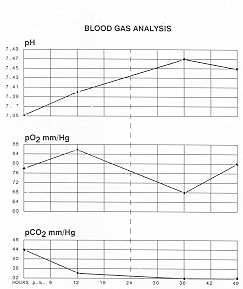
E. Blood gas analysis (Fig. 8) A mild metabolic acidosis was a common
observation, especially during the first 3 post-bum hours. The combination of Ringer's
lactate with an enrichment of NaHC03 resulted in a final stabilization of the pH within
the first 24 hours, which remained also normal during the second day.
Discussion Since Coop and Moore (1942) the goal
of burn resuscitation has been to maintain adequate tissue perfusion, which has been
achieved by the previously proposed formulae of Evans, Mount Vernon, Brooke etc. The
investigations of Moyer et al. and Baxter brought to light the importance of the
sodium/potassium pool and the contrib~tion of the Na+ ion in the intra- and extracellular
distribution of electrolytes and water. This led to the differentation in the conception
of the administration of crystalloid solutions in the initial period of burn shock
resuscitation. Thus, we adopted the use of crystalloid solutions according to the Parkland
formula, since it is based upon the pathophysiology of bum disease by supplying an
adequate amount of sodium during the first 24 hours.
The only disadvantages observed, chiefly in extensive burns, are:
RESUME. Dans une période de deux ans (1987/88), 180 patients avec brûlures en phase aiguë ont été hospitalisés dans notre clinique, dont 64 (35.5%) avec lésions considérées graves (brûlures en plus de 25% de la surface corporelle) qui avaient besoin de réanimation liquide. Cette série incluait tous les patients hospitalisés, indépendamment de l'âge, des lésions concomitantes ou des maladies préexistantes. Pour la réanimation initiale la formule de Parkland a été utilisée comme guide réanimatoire. Cette formule prévoit l'emploi seul du lactate de Ringer dans la première période de 24 heures, avec l'administration d'une quantité de 4 ml/kg/% BSA. Dans la second période de 24 heures elle emploie le plasma dans la mesure de 0.5 ml/kg/% BSA et le glucose à 5% en quantité suffisante pour maintenir une production urinaire adéquate. Après la réanimation initiale les liquides ont été limités aux solutions de maintenance. L'éfficacité de cette thérapie initiale a été évaluée en déterminant: a) la précision des guides réanimatoires; b) la réponse des divers systèmes organiques (systèmes cardiovasculaire, urinaire et pulmonaire, équilibre des liquides et des électrolytes; c) la mortalité précoce; d) les complications rencontrées pendant l'entière première semaine après la brûlure. Selon les résultats exposés la formule de réanimation de Parkland permet une production urinaire suffisante, réduit le développement de l'oedème et en accélère la regression. Elle minimise ainsi le risque de l'insuffisance rénale et de l'oedème cérébrale. Elle est utile pour établir un bon équilibre électrolytique et son coût est inférieur à celui des autres formules. Par contre, elle nécessite une grande quantité de liquides, ce qui requiert un travail d'équipe bien organisé en collaboration avec les infirmiers et un monitorage attentif des paramètres cliniques et de laboratoire pour le contrôle de l'infusion massive des liquides. BIBLIOGRAPHY
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||