| Annals of the MBC - vol. 2 - n' 2 - June 1989
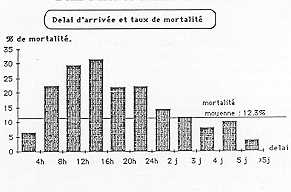
TRANSPORTATION OF BURN PATIENTS Marichy J., Vaudelin Th., Marin-Laflltche I., Gueugniaud P.-Y., Bouchard C1. Centre de Brûlés, Hôpital Edouard Herriot, Lyon, France SUMMARY. It is nowadays well known that an appropriately instituted first aid and medical transport can be important in minimizing the morbidity and the mortality from bum injury. In a recent study we analysed the mortality rate in relation with the transportation of the burned patients admitted to our Bum Centre. Despite the fact that around 60% of the burned patients have a medical transport, the mortality rate remains high (30%) when the patient is admitted between the fourth hour and the twenty-fourth hour after trauma. This fact emphasizes the need to conduct an educational programme not only for the non-medical population but above all for medical and paramedical teams. Introduction In 1979, one year after the Los
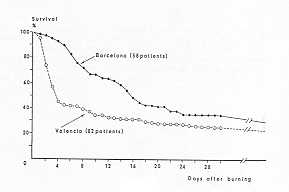
Alfaques disaster, Arthurson and Banuelos reported in their analysis a higher survival
rate in the patients transported to Barcelona than in the patients transported to Valencia
(Fig. 1). There were no significant difterences between the two groups of patients
transported to Barcelona and Valencia with regards to the patients' age and the
seriousness of their bums. The only difference was that the patients taken to Barcelona
received adequate medical treatment during their transportation, unlike most of the
patients taken to Valencia. 1. Population
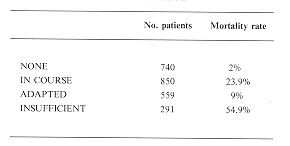
2. Mode of transportation
3. Mortality rate and transportation The mortality rate was lower in the
initial transportation group than in the secondary transportation group (20.3% vs. 26.7%).
It was nil in the private modes group. In eflect, the mean seriousness of the burn was
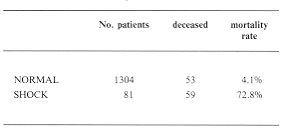
more important in the secondary transportation group. 4. Patients' conditions at admission a) Haemodynamic status At admission, 1304 patients were
considered as having a good haemodynamic status (arterial pressure greater than 1Omm/Hg,
diuresis greater than lml/hr., central venous pressure greater than 0, no
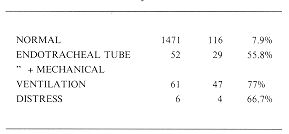
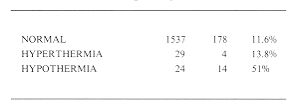
vasoconstriction); 4.1% of the patients died (Fig. 3). b) Pulmonary function Amongst the population having no clinical sign of inhalation injury (1471 patients), there were 116 fatalities due to the seriousness of the burns and septic complications (7.9%). Nevertheless, in this population it is possible that some patients had an inhalation injury without any clinical sign. Early complication of inhalation injury appeared in 119 patients; 80 of these died (67.2%). In a more recent study on 582 patients admitted to our Bum Centre from January 1984 and December 1985, the mortality rate of these patients was lower (50%) (Fig. 5). c) Thermoregulatory status Despite the fact that information about the ill-regulated function of the burned patient is widespread, 24 patients were hypothermic at their admission, and 14 died (58%). Their rectal temperature was below 35' (Fig. 6). d) Neurological signs The neurological status was classified according to the Glascow score, ranging from 15 (normal) to 0 (coma). The mortality rate was low for patients having a Glascow score of 15 (3.5%), compared to patients with a score below 10 (66.7%) or under anaesthesia (51.9%) (Fig. 7).
5. Discussion Two identified phases of transportation of burn patients are the initial transfer from the scene of the accident to the nearest hospital and the referral of the burn patient from this hospital to the regional bum centre. In both cases, an adequate transportation must be planned according to instituted rules: A) Management of the burn patient before transportation
B) Local treatment
6. Conclusions All these rules are well known by the
Bum Centres but are sometimes neglected by physicians and/or paramedics working in a
general hospital or even in the hospital where the Burn Centre is located. In the majority
of cases, a single call to the specialist may solve a delicate problem. RESUME. La prise en charge précoce du brûlé est un élément capital pour sa survie. L'évolution parallèle des techniques de réanimation et la structuration des organisations publiques (S.A.M.U.) et privées de transport devraient contribuer à diminuer les taux de morbidité et de mortalité des brûlés. Dans une étude rétrospective portant sur 1532 brûlés hospitalisés entre 1978 et 1983 au Centre de Brûlés de l'Hôpital Edouard Herriot, nous avons analysé le taux de mortalité en fonction des conditions de transport des patients et de la précocité de celui-ci. Les résultats indiquent que des efforts d'information auprès des équipes médicales et paramédicales sont encore nécessaires pour améliorer la prise en charge initiale du brûlé. |