Annals qf the MBC - vol. 2 - n* 2 - June 1989 THE USE OF TISSUE EXPANSION FOR RECONSTRUCTION OF POST-BURN ALOPECIAZaki M.S. Plastic Surgery Unit, Faculty of Medicine, Cairo University, Egypt SUMMARY. Controlled tissue expansion was used for scalp reconstruction in ten patients with post-burn alopecia. The time between the bum injury and reconstruction ranged between 3 and 21 years. Expanders with a remote valve were used in this series. They were introd ' uced either through a remote incision or by a paralesional approach. Multiple expanders were used when the dimensions of the defect exceeded 10 x 18 cm. The expanders were serially filled starting two to three weeks post-operatively. The expansion was carried out usually twice per week, guided by both patient tolerance and tissue response. The end of the expansion period is reached when the measured length of the expanded flaps can give the needed advancement to reconstruct the scalp defect. The clinical results showed that tissue expansion is an ideal technique for reconstruction of post-burn alopecia, and it has several advantages over other surgical procedures. Introduction Treatment of large areas of post-burn
alopecia constitutes a real problem for the reconstructive surgeon. The conventional
methods of rotational scalp flaps, serial excision, microvascular flap transfer and free
hair transplantation have many drawbacks including lengthy hospital stays, flap necrosis
and inability to cover major scalp defects (1, 2, 3,). Recently, the introduction of
controlled tissue expansion to treat scalp defects has started a new era of reconstruction
(4,5). Patients and methods Ten patients with post-burn alopecia were treated by tissue expansion, 6 females and 4 males. Their ages ranged between 5 and 25 years. The time between the bum injury and reconstruction ranged between 3 and 21 years. The surface area of alopecia was 20-40% of the total hair-bearing scalp. Surgical technique Pre-operative measurement of the
defect and donor site selection of non-involved areas of hair-bearing scalp were evaluated
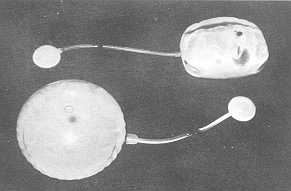
for every patient. Expanders with a remote valve, both rectangular and rounded, were used
in this series (Fig.1).
A pocket in the subgaleal space about 1 em
larger than the expander base was created to accommodate the expander. The remote valve
was embedded within the subcutaneous tissue of the lateral neck, at least 5 em away from
the expander, and was easily palpable. The integrity of the expander was then tested by
injecting about 50 cc sterile saline. This amount of saline was usually left in the
expander to allow obliteration of any dead space and prevent haematoma collection. Lastly,
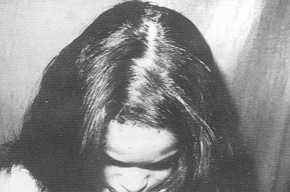
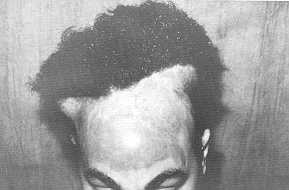
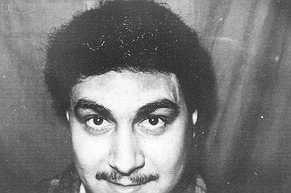
the wound was closed with a suction drainage which was removed after 24-48 hours. Results In the series, it was possible to
completely reconstruct the scalp defects of 7 patients (70%) after the two stages, using
tissue expansion (Fig. 2, 3). In the remaining 3 patients, additional scalp flaps or
re-expansion were needed to reconstruct residual areas of alopecia.
Discussion There is no tissue in the human body
which can effectively simulate lost scalp (4). The introduction of controlled tissue
expansion in the treatment of scalp defects is thus considered to be a breakthrough in
reconstructive surgery. The use of this technique for the treatment of post-burn alopecia
has been reported (5).
Concerning the age of patients, delay of
the operation till the age of 5 years is recommended in order to avoid the possible
complication of pressure necrosis of the skull bones and to be able to communicate easily
with the older child. RÉSUMÉ. L'expansion contrôlée tissulaire a été utilisée pour la reconstitution du cuir chevelu chez 10 patients avec alopécie à la suite de brûlure. Le temps passé entre la lésion thermique et la reconstitution variait de 3 jusqu'à 21 ans. Dans cette série nous avons utilisé des expanseurs avec valve à distance ou une approche paralésionelle. Quand la partie intéressée a les dimensions supérieures à 10 x 18 cm, nous avons utilisés les expanseurs multiples. Les expanseurs; ont été remplis en série à partir de 2 ou 3 semaines après l'acte opératoire. L'expansion a été effectuée normalement deux fois par semaine, selon la tolérance du patient et la réponse tissulaire. La phase de l'expansion est terminée dès que la longueur mesurée des lambeaux en expansion est suffisante pour reconstituer le défaut du cuir chevelu. Les résultats cliniques ont montré que l'expansion tissulaire est une technique idéale pour la reconstitution de l'alopécie à la suite de brûlure qui offre plusieurs avantages par rapport à d'autres procédures chirurgicales. BIBLIOGRAPHY
|
|||||||||||||||||||