Annals of the MBC - vol. 2 - n' 3 -
September 1989
IONTOPHORESIS IN THE TREATMENT OF BURN EAR CHONDRITIS
Peled 1.j., Zagher U., Rotem M.
Dept. Plastic and Maxillofacial Surgery, Hadassah
University Hospital, Jerusalem, Israel
SUMMARY. Burn chondritis of the
ear is quite a common complication with difficult treatment and poor aesthetic results. We
report the use of preventive and therapeutic iontophoresis with gentamicin and using a
custom-made acrilic resin stent. This modality of treatment has rendered gratifying
results and lessened the need for surgical procedures.
It is well known that in large bums 60% of
the victims have burns of the face and ears. While healing of the face is fairly
satisfactory in most cases, problems arise with burned ears. Because of the anatomical
structure and the lack of vascularization of the cartilage (1), burned ears are often
complicated with chondritis, which can present in a wide range of severity from redness to
severe necrosis, with clinical behaviour similar to malignant external otitis.
The classical treatment of this condition can be divided into conservative, which
represents mainly prophylaxis, and surgical, which may consist in drainage and debridement
up to radical excision of the involved cartilage, with significant residual deformity (2).
Success will depend on starting the treatment at an early stage. Once the golden hours are
gone the outcome may be auto- or surgical amputation.
Several topical treatments have been tried for burn chondritis, namely topical ointment,
creams and local injections of antibiotics (3) with results falling short of expectation.
We would like to report our experience in the use of iontophoresis in the prevention and
treatment of car chondritis.
Technique
The current was supplied by a 45 V dry
cell battery which generated a current up to 20 mAmp, regulated with a 25000 ohms
potentiometer.
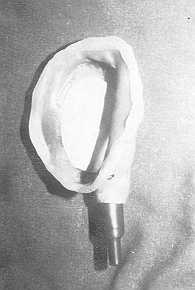
A gauze soaked in gentamicin sulphate solution, 80 mg/cc, was placed over the effected
auricle. The active electrode was incorporated in the custom-made acrilic-resin stent (4)
(Fig. 1-2).
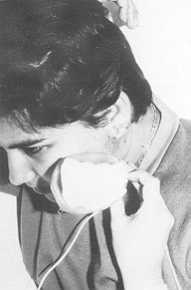
A current of 2-5 mAmp was applied twice a day, 30 minutes each time, for 10 days to two
weeks (Fig. 3). The antibiotic we chose was gentamicin because of its charge and its
activity against the most common bacteria, Pseudomonas aeruginosa and Staphylococus aureus
(2). The patients showed local improvement as soon as 2 days after the beginning of the
treatment.
 |
 |
| Fig. 1: Custom-made
acrilic resin stent with the active elecrode incorporated. |
Fig. 2: Gentamicin
soaked gauze between the active electrode and the atTected car. |
 |
 |
| Fig. 3: Treatment
with iontophoresis twice daily, 30 minutes each. |
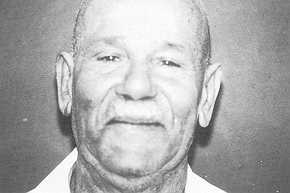
Fig. 4: Complete
healing in 10 days. |
|
Discussion
Iontophoresis is the migration of
charged ions in an electrical field.
In 1908, Leduc (5) reported the medical use of iontophoresis for the introduction of drugs
into the body and it was shown that chemicals could be carried across an avascular
membrane using direct current as the transporting agent.
In 1965, Rapperport (6) using iontophoresis achieved a very high level of penicillin in
eschar. In 1978 and 1980 iontophoresis was clinically used for the treatment of ear
chondritis (7).
In order to assess the levels of gentamicin in the cartilage of the ear an experimental
work was done in rabbit ears treated with iontophoresis using various currents. The
results showed very high levels of gentamicin in the cartilage, up to 200 times as high as
that obtained by intravenous injections (unpublished data). Systemic administration of
antibiotics fails to produce bactericidal levels in the cartilage due to the avascularity
of the tissue (8). In our experience prophylactic and therapeutic antibiotic lontophoresis
significantly diminished auricular chondritis in the burned patient (Fig. 4-5). It should
be stressed that prevention or very early treatment of the aacted ear will often obviate
the surgical treatment and resulting deformity.
Patients with ongoing infection had a rapid relief of the symptoms following 3 or 4
sessions of iontophoresis. It is also important to keep in mind that in more severe cases
iontophoresis will not obviate the need of surgical wound care but will become part of the
treatment together with avoidance of pressure, cleansing and debridement of necrotic
tissue.
RÉSUMÉ. La chondrite de l'oreille à la
suite de brûlure est une complication non rare, difficile à traiter et avec des
résultats esthétiques insuffisants. Nous décrivons l'emploi de l'ionophorèse
préventive et thérapeutique avec gentamicine, utilisant un stent de résine acrylique
fait sur mesure. Cette méthode de traitement a donné des résultats satisfaisants et a
diminué la nécessité d'actes operatoires.
BIBLIOGRAPHY
- Grant D., Finley M.L., Coers C.R.: Early management
of the burned ear. Plast, Reconstr. Surg. 44: 161, 1969.
- Dowling J.A., Foley F.D., Moncrief J.A.: Chondritis
in the burned car. Plast. Reconstr. Surg. 42: 115, 1968.
- Apfelberg D.B., Waisbren B.A., Masters F.W.,
Robinson D.W.: Treatment of chondritis in the burned ear by local instillation of
antibiotics. Plast. Reconstr. Surg. 53: 179, 1974.
- Sela M., Peled I., Zagher U., Taicher S.:
Maxillofacial prosthetics and iontophoresis in management of burned ears. J. Prosth Dents.
7: 226, 1985.
- Leduc S.: "Electronic ions and their use in
Medicine". Mcbman Ltd., London, 1908.
- Rapperport A.S., Larson D.L., Henges D.F., Lynch
J.B., Blocker T.G., Lewis R.S.: lontophoresis: a method of antiobiotic administration in
the burned patient. Plast. Reconstr. Surg. 36: 546, 1965.
- Laforest N.T., Cofrancesco C.: Antibiotic
iontophoresis in the treatment of ear chondritis. Phys. Ther. 58: 32, 1978.
- Greminger R.F., Elliot R.A., Rapperport A.S.:
Antibiotic iontophoresis for the management of the burned ear chondritis. Plast. Reconstr.
Surg. 66: 356, 1980.
|